Doctor Children's Hospital of Fudan University Shanghai, Shanghai, China (People's Republic)
Background: While caspofungin is increasingly used to treat invasive fungal infections in critically ill children, its pharmacokinetic profile in this population remains poorly understood, and current dosing regimens are not firmly supported by scientific evidence. This study aimed to characterize the population pharmacokinetics of caspofungin in critically ill children and to identify dosing strategies most likely to achieve optimal therapeutic exposure. Objective: To develop a population pharmacokinetic model describing both total and unbound caspofungin concentrations in critically ill children; to evaluate and optimize the application of current standard treatment dosing regimen. Design/Methods: This was a prospective, observational clinical study of intravenous caspofungin administered to children in PICU for the treatment or prophylaxis of fungal infections (NCT04961593). The standard dosing strategy based on body surface area (BSA) using the Mosteller formula was adopted: loading dose of 70 mg/m² on the first day, followed by 50 mg/m² daily for maintenance. The PopPK model was developed using the NONMEM (version 7.5.0) with theFOCE-I algorithm. Results: A total of 29 children were enrolled in the study, with 138 concentrations for both total (0.155-58.3 mg/L) and unbound (0.00305-2.11 mg/L) caspofungin. The median (range) age and weight are 5.33 years (0.33-16) and 16 kg (4.9-74). Four patients underwent ECMO during caspofungin treatment. A total of 138 plasma samples collected from 29 pediatric patients (0.33-16 years) were included in final analysis. The two-compartment model with allometric scaling on BSA, exponential 1 for volume of distribution and 0.66 for clearance accurately described time courses of caspofungin. Extracorporeal membrane oxygenation significantly increased the central volume of distribution (effect coefficient 18.2), but there was no significant difference in area under the concentration curve (AUC) between patients with and without ECMO support. Simulations indicated a BSA cut-off of 1.4 m², suggesting that a fixed maintenance dose (MD) is more appropriate for patients with BSA ≥ 1.4 m², while the standard BSA-based MD remains preferable for those with BSA < 1.4 m². If Cmin,ss was the target, patients receiving ECMO would require higher doses for adequate exposure.
Conclusion(s): Our study proposed optimized caspofungin dosing based on tAUCss,24h/MIC or Cmin,ss, supporting precision treatment and addressing the research gap in critically ill pediatric ICU patients, especially those on ECMO.
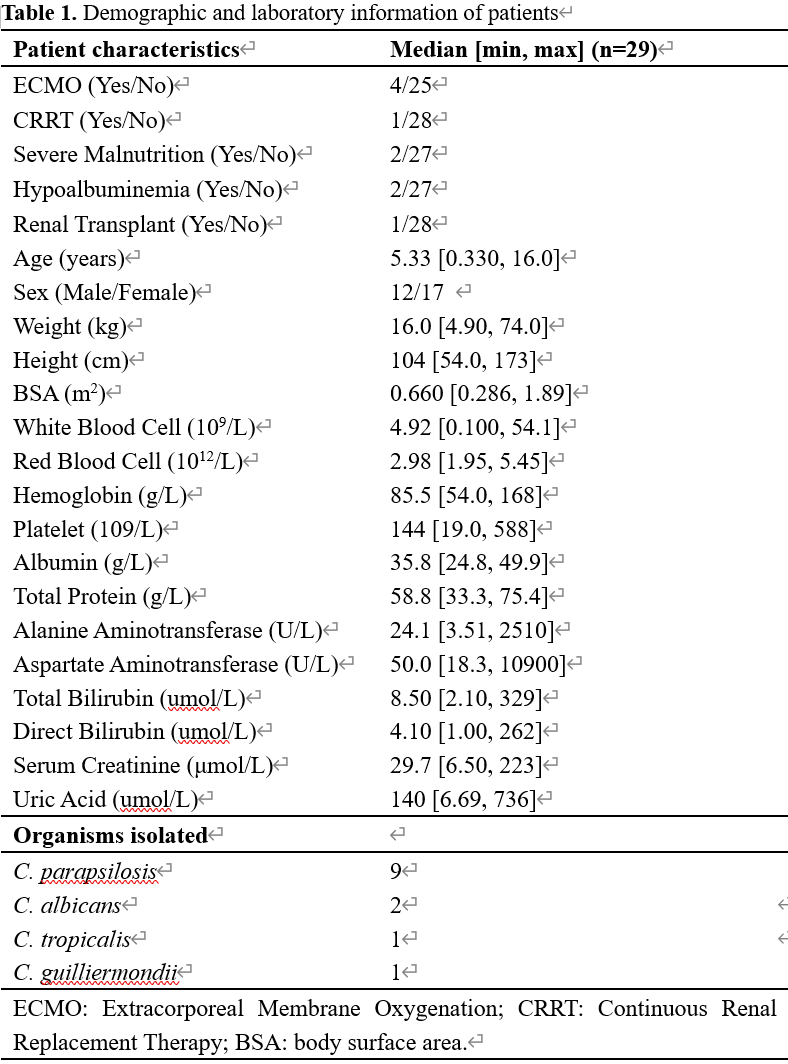
Demographic and laboratory information of patients
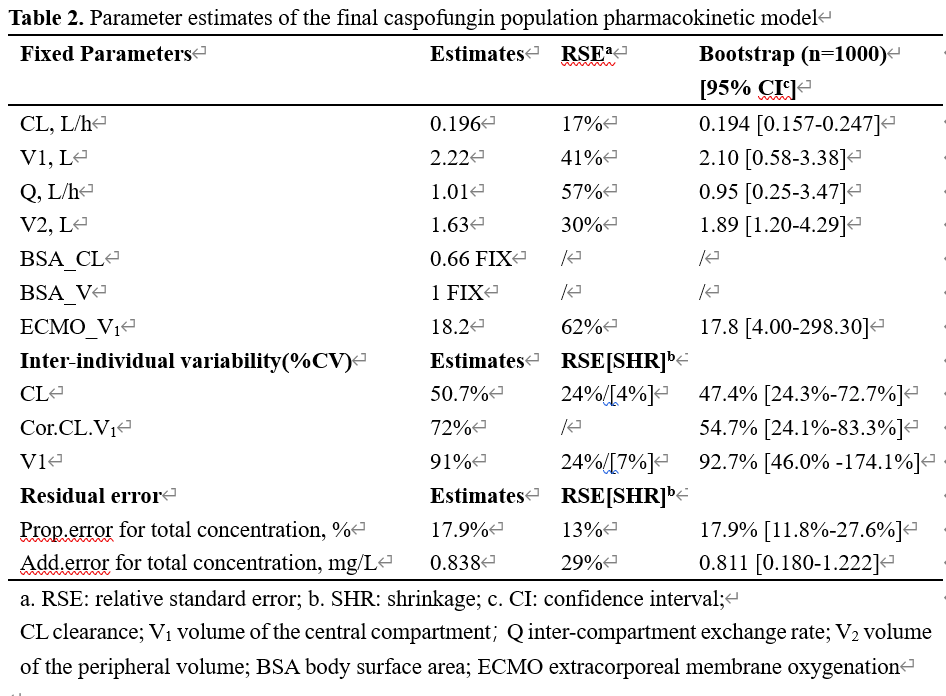
Parameter estimates of the final caspofungin population pharmacokinetic model
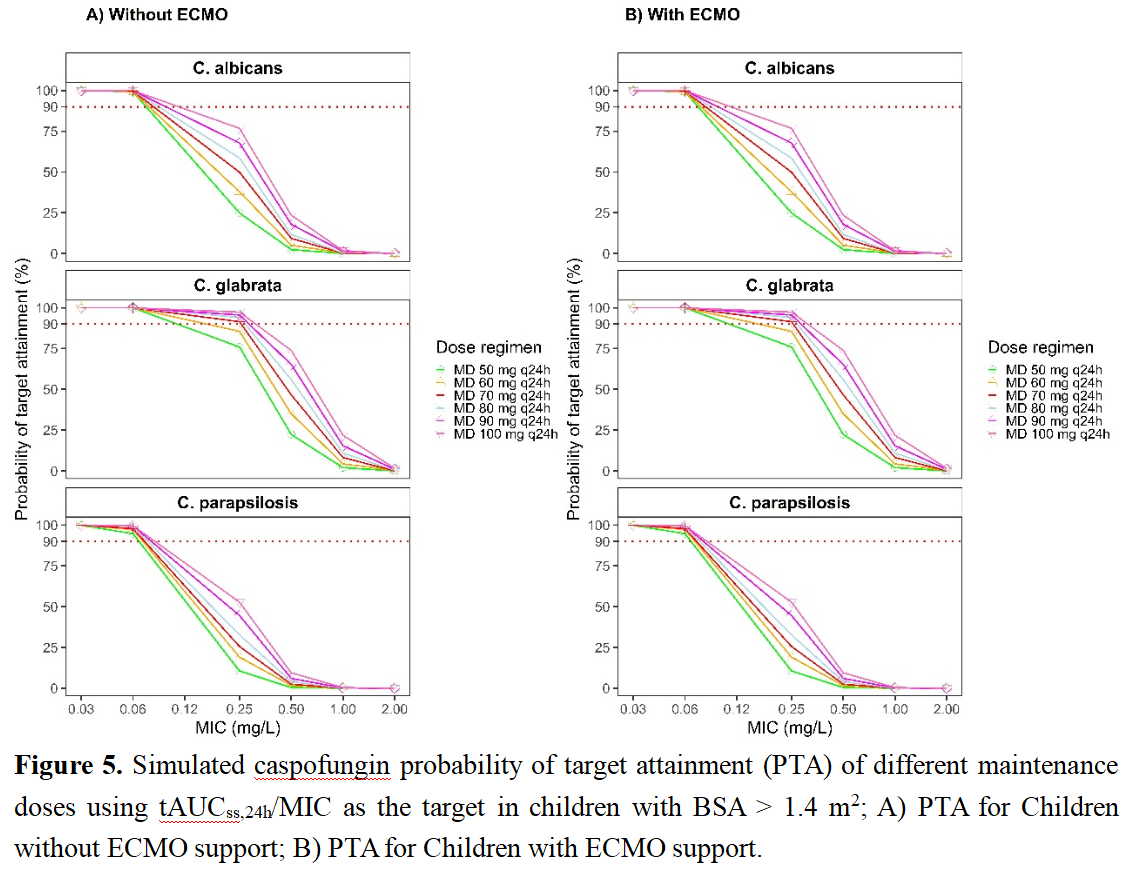
Simulated caspofungin probability of target attainment (PTA) of different maintenance doses using tAUCss,24h/MIC as the target in children with BSA > 1.4 m2