409 - Development and Validation of a Cuff Size Prediction Model for Pediatric Blood Pressure Measurement Outside the Office
Friday, April 24, 2026
5:30pm - 8:00pm ET
Publication Number: 1392.409
James T. Nugent, Yale School of Medicine, New Haven, CT, United States; Victoria Cueto Vilorio, Yale School of Medicine, New Haven, CT, United States; Hugh M. Medvecky, The Warren Alpert Medical School of Brown University, Providence, RI, United States; Morgan T. Harper, Yale School of Medicine, Boston, MA, United States; Jason H. Greenberg, Yale School of Medicine, New Haven, CT, United States; Veronika Shabanova, Yale School of Medicine, New Haven, CT, United States
Assistant Professor of Pediatrics Yale School of Medicine New Haven, Connecticut, United States
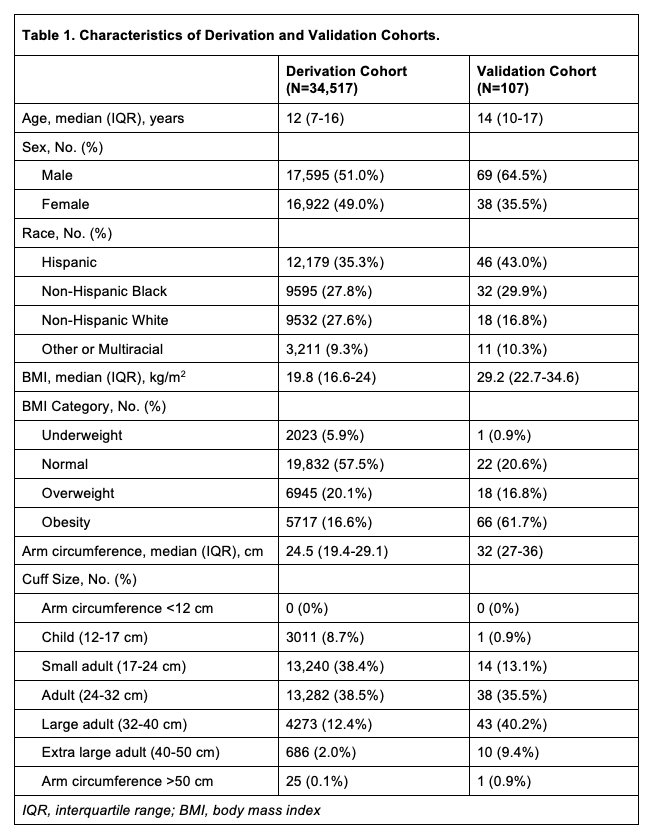
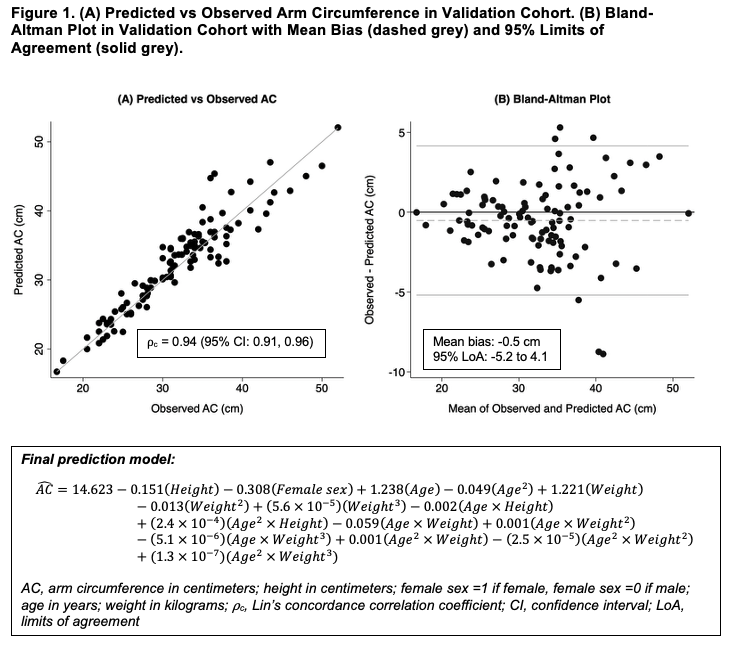
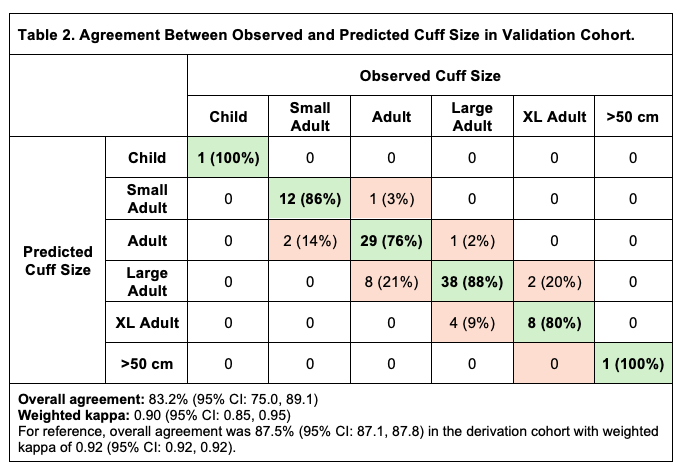
Background: Pediatric guidelines recommend ambulatory blood pressure monitoring (ABPM) outside the clinic to diagnose hypertension. However, in-person clinic visits are necessary to measure mid-arm circumference (AC) and determine the appropriate cuff size for ABPM. Objective: To develop and validate a model to predict AC and BP cuff size in youth undergoing evaluation for hypertension using readily available data from the electronic health record. Design/Methods: We developed a prediction model for youth aged 3-21 years using data from the 1999-2018 National Health and Nutrition Examination Survey. Using linear regression, we considered piecewise and polynomial effects of age, sex, height, and weight as candidate predictors of AC. We selected the most parsimonious model with the highest adjusted R2, lowest bootstrapped root mean square error (RMSE), and lowest predicted residual error sum of squares (PRESS) with leave-1-out cross-validation. We validated the model in an external cohort of youth with AC measured in the pediatric hypertension clinics at an academic medical center in the Northeast. We used Lin's concordance correlation coefficient (⍴c) for observed and predicted AC, and Bland-Altman plots to evaluate mean bias and 95% limits of agreement (LoA) in AC. We assessed categorical agreement between the observed and predicted cuff size using Cohen's weighted kappa with 95% confidence intervals (CI). Results: Based on 34,517 youth in the derivation cohort (12 years [IQR: 7, 16], 49.0% female, 16.6% obesity) (Table 1), the final model included age, age2, sex, height, weight, weight2, weight3, and all-possible interactions between age and height and between age and weight (adjusted R2: 0.97, RMSE: 1.20, PRESS: 49,417). In the external validation cohort of 107 youth (14 years [IQR: 10, 17], 35.5% female, 61.7% obesity), observed and predicted AC were highly concordant (⍴c: 0.94 [P < 0.001]) with a mean bias of -0.5 cm (95% LoA: -5.2, 4.1) (Fig 1). Overall agreement for selecting the appropriate cuff size was 87.5% (95% CI: 87.1, 87.8) in the derivation cohort with weighted kappa of 0.92 (95% CI: 0.92, 0.92) and 83.2% (95% CI: 75.0, 89.1) in the validation cohort with weighted kappa of 0.90 (95% CI: 0.85, 0.95) (Table 2).
Conclusion(s): Although direct measurement of AC is the gold standard for selecting an appropriate BP cuff size, we found substantial agreement between the observed and predicted AC from a model using basic information available in the electronic health record. This model may be used to facilitate BP monitoring outside the clinic for telehealth visits or when in-person visits are not feasible.
Table 1. Characteristics of Derivation and Validation Cohorts.
Figure 1. (A) Predicted vs Observed Arm Circumference in Validation Cohort. (B) Bland-Altman Plot in Validation Cohort with Mean Bias (dashed grey) and 95% Limits of Agreement (solid grey).
Table 2. Agreement Between Observed and Predicted Cuff Size in Validation Cohort.

 photo")