571 - Improving the Incidence of Patient Gowning in the Pediatric Emergency Department
Friday, April 24, 2026
5:30pm - 8:00pm ET
Publication Number: 1548.571
Jacob A. Klinger, Mayo Clinic Children's Center, Rochester, MN, United States; Olivia E. Stanier, Mayo Clinic Children's Center, Rochester, MN, United States; John Anderson, Mayo Clinic Children's Center, Rochester, MN, United States; Erin Larson, Mayo Clinic, Rochester, MN, United States; Kimberly Goergen, Mayo Clinic, Rochester, MN, United States; Cree Kachelski, Mayo Clinic Children's Center, Rochester, MN, United States; Meghan Cain, Mayo Clinic Children's, Rochester, MN, United States
Emergency Medicine Medical Scribe Mayo Clinic Children's Center Rochester, Minnesota, United States
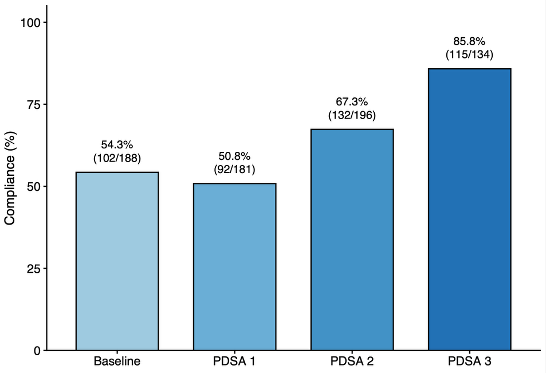
Background: Patient gowning is essential in pediatric emergency assessment, allowing for comprehensive evaluation of rashes, perfusion, respiratory effort, trauma, and maltreatment. Gowning is especially critical in children under four years, when full exposure is necessary to assess for signs of physical abuse. In 2021, our institution implemented a guideline to standardize gowning in the pediatric emergency department (ED), but there was notably low compliance. Objective: This quality improvement project aimed to increase compliance with our gowning guideline from a baseline rate of 54.3% to 70% without adversely impacting length of stay (LOS). Design/Methods: Baseline data were prospectively collected by direct observation by an ED medical scribe across 2.5 months. Of 221 patients, 188 met gowning criteria by the guideline and 54.3% (102/188) were appropriately gowned. A root cause analysis identified key causes including: limited awareness of the guideline, uncertainty about gowning's importance, and ease of access to gowns. Interventions were implemented through three Plan-Do-Study-Act (PDSA) cycles. PDSA 1: A visual flowchart outlining gowning indications was posted in all pediatric rooms to improve visibility. PDSA 2: Education emphasizing the role of gowning in complete assessments and maltreatment detection was completed using the Awareness, Desire, Knowledge, Ability, Reinforcement (ADKAR) framework. PDSA 3: Adding a stock of gowns to the patient scale area to support access. Results: During PDSA 1, 235 encounters were observed, of which 181 patients met gowning guideline criteria. Compliance with internal gowning guidelines decreased to 50.8% (92/181, p= 0.41). During PDSA 2, 249 encounters were observed, with 196 in-scope of the guideline. Gowning compliance improved to 69.5% (132/196) among visits that met gowning criteria, a statistically significant (p < 0.01) relative increase from baseline. With PDSA 3, 134 of the 184 observed encounters met criteria for gowning. 85.8% (115/134) of these patients were gowned. This represented a 68.9% relative improvement from baseline (p < 0.01). LOS was not significantly different from baseline to PDSA 3 (169 minutes versus 172 minutes, p= 0.803).
Conclusion(s): Targeted education and access to materials significantly improved adherence to pediatric gowning guidelines in the ED. Measurable change required clear guidance, regular feedback, and multidisciplinary engagement. The ADKAR-based approach enhanced staff buy-in, reinforcing that behavioral and cultural shifts are key to embedding quality and safety practices into clinical workflow.
Figure 1. Pediatric emergency department gowning compliance by Plan-Do-Study-Act cycle.