693 - Bowel Ultrasound in Very Low Birth Weight Infants with Necrotizing Enterocolitis: Single-Center Cohort Study
Friday, April 24, 2026
5:30pm - 8:00pm ET
Publication Number: 1670.693
Thomas C. Lu, Baylor College of Medicine, Houston, TX, United States; Elena Itriago, Baylor College of Medicine, Houston, TX, United States; Laura Gollins, Texas Children's Hospital, Houston, TX, United States; Joseph Hagan, Baylor College of Medicine, Houston, TX, United States; Martha M. Munden, Texas Children's Hospital, Houston, TX, United States; Pamela Ketwaroo, Texas Children's Hospital, Baylor College of Medicine, Orange, CT, United States; Muralidhar H. Premkumar, Baylor College of Medicine, Houston, TX, United States; Mohan Pammi, Baylor College of Medicine, Bellaire, TX, United States; Adam M.. Vogel, Texas Children's Hospital, Houston, TX, United States; Amy B. Hair, Baylor College of Medicine, Houston, TX, United States
Neonatal-Perinatal Medicine Clinical Fellow Baylor College of Medicine Houston, Texas, United States
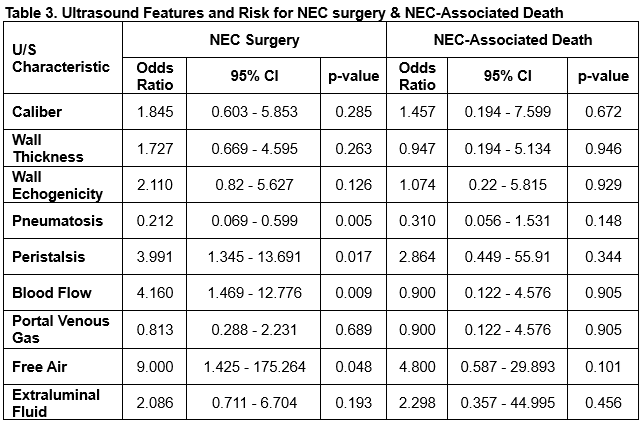
Background: Necrotizing enterocolitis (NEC) affects 2-10% of very low birth weight infants (VLBW) in the neonatal intensive care unit (NICU) and has a high mortality rate. Currently, providers rely on nonspecific clinical and radiographic data, which may lead to delayed diagnosis or unwarranted antibiotic exposure. Abdominal ultrasounds (US) have been increasingly used for the diagnosis of NEC. Objective: Assess the agreement between US and radiographs in detecting NEC, and to examine the correlation of US findings with surgery and mortality in VLBW infants with NEC. Design/Methods: This single-center retrospective study examined VLBW preterm infants admitted to a quaternary NICU from 2015 to 2024 with NEC as defined by the Vermont Oxford Network and an US study at the time of the NEC episode of interest. All US were reviewed by an experienced radiologist. Logistic regression was used to analyze the relationship between US findings, NEC surgery, and NEC-related mortality. Results: A total of 72 infants were analyzed. Using radiographs as the gold standard, an evaluation of US performance showed a sensitivity of 77% and positive predictive value of 38% for detecting pneumatosis, portal venous gas, or free air. US and radiographs identified pneumatosis in 68% vs. 35% of patients, respectively (p < 0.001). On US, abnormalities in bowel wall thickness, wall echogenicity, peristalsis, blood flow, and presence of free fluid were linked to longer NPO and antibiotic durations. US-detected pneumatosis was associated with lower odds of surgery (odds ratio [OR] 0.21, 95% confidence interval [CI] 0.07-0.60, p=0.005). However, signs of abnormal peristalsis (OR 3.99, 95% CI 1.35-13.69, p=0.017), abnormal blood flow (OR 4.16, 95% CI 1.47-12.78, p=0.009), and pneumoperitoneum (OR 9.00, 95% CI 1.43-175.26, p=0.048) were linked to a higher likelihood of surgery. Radiographic pneumatosis and portal venous gas did not correlate with surgery. No significant associations were found between US findings with mortality from NEC.
Conclusion(s): US detected pneumatosis more often than radiographs, and US pneumatosis was linked to a lower chance of needing NEC surgery, possibly due to earlier detection and treatment. Additionally, some US features have the potential to identify cases with higher risk of surgery. Observed US associations were based on retrospective expert review and may not represent information used for real-time decisions. In the future, the neonatal Sequential Organ Failure Assessment, a validated tool in predicting the need for surgery or mortality in NEC, will be integrated to create a new tool for evaluating NEC.
Characteristics of Cohort
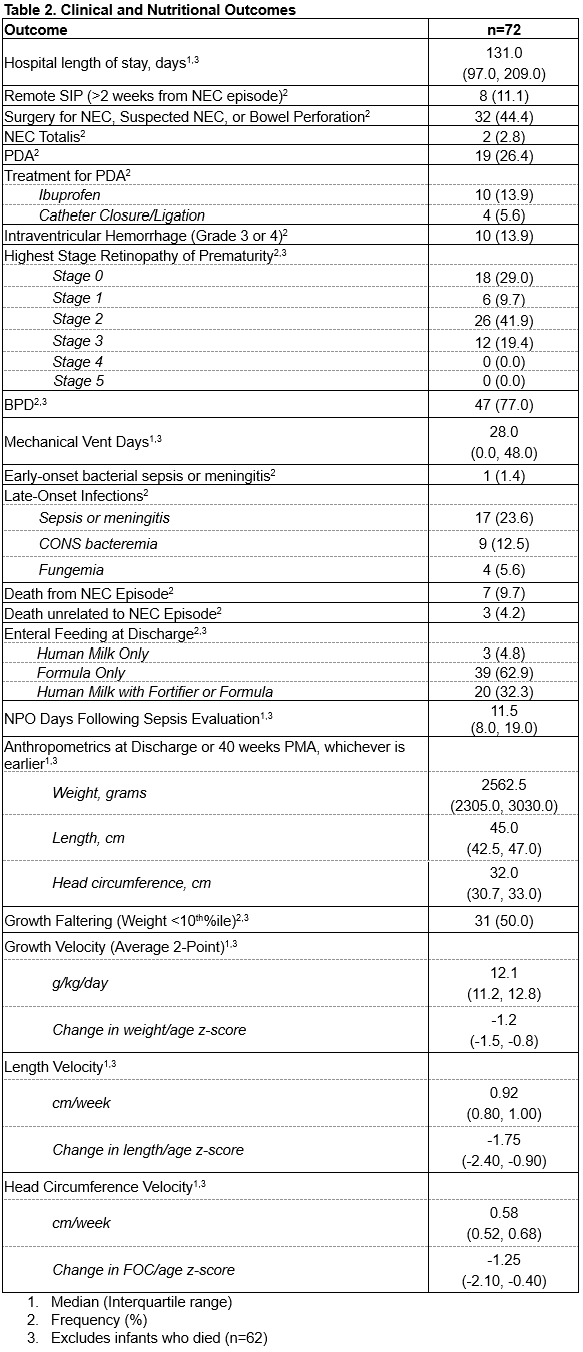
Clinical and Nutritional Outcomes
Ultrasound Associations with NEC Surgery and NEC-Related Death

 photo")
.png)