556 - Intensivist Workload Stratified by Level of Care: National Survey of United States Pediatric Intensivists
Friday, April 24, 2026
5:30pm - 8:00pm ET
Publication Number: 1535.556
Nicholas Ettinger, Children's Healthcare of Atlanta/Emory University School of Medicine, Atlanta, GA, United States; Benson Hsu, University of South Dakota, Sanford School of Medicine, Sioux Falls, SD, United States; Paul A. Licht, Boston Children's Hospital, Allston, MA, United States; David Wypij, Boston Children's Hospital, Boston, MA, United States; Karen E.A.. Burns, Unity Heslth Tironto, Tirinto, ON, Canada; Michael Agus, Harvard Medical School, Boston, MA, United States
Pediatric Intensivist/Fellowship Program Director Children's Hospital of Georgia Atlanta, Georgia, United States
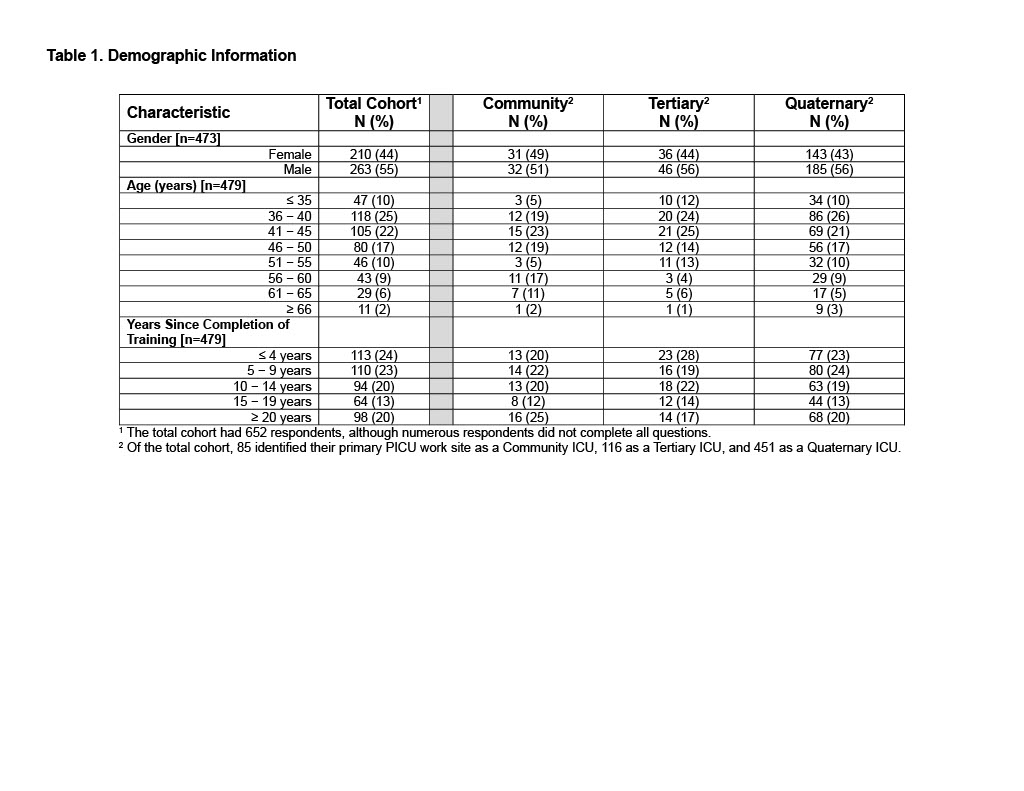
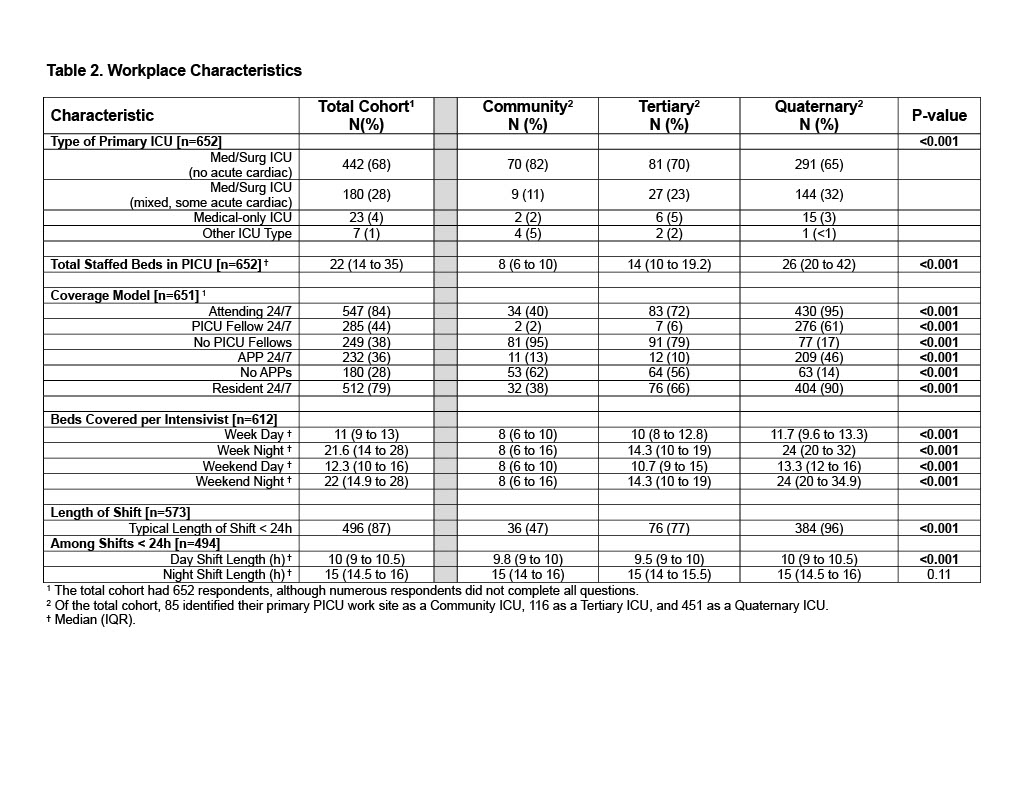
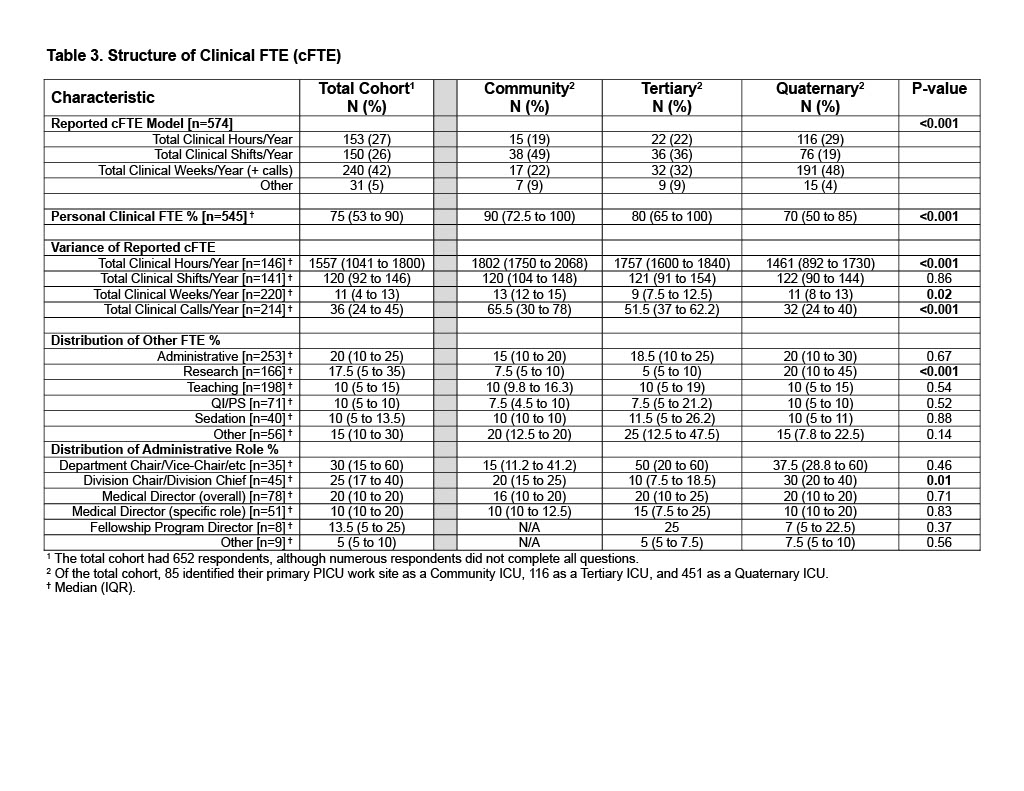
Background: In a 2020-2022 survey of pediatric critical care division chiefs and medical directors, we identified that a 1.0 clinical FTE (cFTE) was most commonly represented by 'total shifts per year' (Ettinger et al, 2024). However, this finding may not reflect the views of practicing pediatric intensivists and may vary by ICU size and/or level of care provided (community vs. tertiary vs. quaternary; Hsu et al, 2019). Objective: To further characterize individual pediatric intensivist's perceptions of their workload and how self-reported workload varied by PICU size and level of care. We hypothesized that pediatric intensivist workload would vary significantly by PICU level of care. Design/Methods: We used a national cross-sectional electronic survey of members of five independent intensivist society and network email mailing lists. We excluded those who worked exclusively in a cardiac ICU, were exclusively part-time, were exclusively employed in locum tenens positions, or were trainees/APPs. Results: Of the 3437 currently ABP-certified pediatric intensivists, we received 765 responses (22%). After deleting duplicate responses, we analyzed 652 responses, although numerous respondents did not answer all questions. Overall, respondents were 44% female and most commonly between 36-45 years [N = 223 (47%)] with less than 10 years of experience [223 (47%)] (Table 1). The majority worked in non-cardiac medical/surgical ICUs [442 (68%)] and had in-house attending coverage 24/7 [547 (84%)] (Table 2). 'Beds covered per intensivist' varied by level of care and essentially doubled at night as compared to day at larger institutions (Table 2). The median duration of day and night shifts were 10 h and 15 h, respectively. The most common reported cFTE model was 'total clinical weeks per year + calls' [n=240, (42%)] with an overall median reported cFTE = 75% [IQR 53%-90%] (Table 3). Although total clinical shifts per year did not vary by PICU level of care among the 141 intensivists with this cFTE model, both total clinical hours per year and total clinical calls per year decreased as level of care increased, likely reflecting a larger labor pool and more protected time for research. Of those who reported working as a division chief, the median reported protected FTE was 25% and the median reported FTE for a PICU medical director was 20%.
Conclusion(s): The most commonly reported cFTE model was total clinical weeks per year plus calls with the median cFTE reported as 75%. However, these models varied across PICU levels of care, likely reflecting different workload distributions among larger numbers of intensivists.

 photo")