Session: Neonatal Pulmonology - Clinical Science 2: Bronchopulmonary Dysplasia II
387 - Outcomes of Extremely Preterm Infants with Severe Bronchopulmonary Dysplasia
Friday, April 24, 2026
5:30pm - 8:00pm ET
Publication Number: 1371.387
Dinushan C. Kaluarachchi, University of Wisconsin - Madison, Madison, WI, United States; Samuel Afah Annah, University of Wisconsin Madison, Madison, WI, United States; Nethan M. Kaluarachchi, Middleton High School, Middleton, WI, United States; Michael R.. Lasarev, University of Wisconsin School of Medicine and Public Health, Madison, WI, United States; Patrick J. Peebles, University of Wisconsin School of Medicine and Public Health, Madison, WI, United States
Student University of Wisconsin Madison Madison, Wisconsin, United States
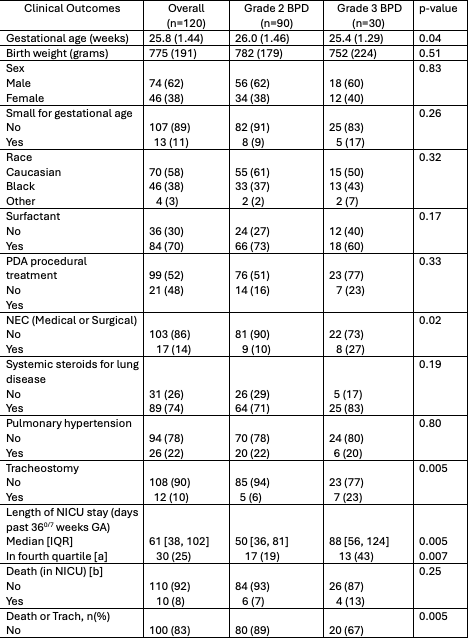
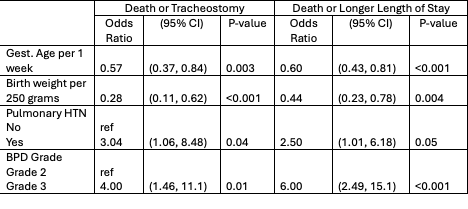
Background: Bronchopulmonary dysplasia (BPD) is a common lung disease in preterm infants that increases the risk of mortality and later-life sequelae such as respiratory insufficiency and abnormal neurodevelopment. Data describing outcomes of preterm neonates with severe BPD is limited, particularly in determining timing for clinical interventions and counseling families. Objective: To describe clinical outcomes of extremely preterm infants with severe BPD (Grade 2-3 BPD according to the definition by Jensen et al) and, to identify predictors of unfavorable outcomes among infants with severe BPD. Design/Methods: This is a retrospective cohort study of preterm infants born at 23 0/7 to 28 6/7 weeks with severe BPD in the Prematurity and Respiratory Outcomes Program. Infants with cardiopulmonary anomalies, non-viable infants, those unavailable for follow-up, those who died prior to 36 week's PMA and those with no BDP or with grade 1 BPD were excluded. Demographic and clinical variables were compared between infants with Grade 2 and Grade 3 BPD. The two unfavorable outcomes were defined as: 1) death or tracheostomy, and 2) death or longer length of stay (4th quartile for length of stay). Odds ratios of patient characteristics, other morbidities, and BPD Grade 2 or 3 for the two unfavorable outcomes were calculated. Results: A total of 120 infants with severe BPD were included. Likelihood of death was unrelated to BPD grade (7% vs 13%, p=0.25). Tracheostomy placement was performed on 7/30 (23%) of those with Grade 3 BPD and 5/90 (6%) of those with Grade 2 BPD (p=0.005). Length of NICU stay was significantly longer for Grade 3 (162 vs 125 days, p=0.003) (Table 1). Grade 3 BPD was associated with higher odds of death or tracheostomy (OR 4.0, CI 1.46, 11.1) and death or longer length of stay (OR 6.0, CI 2.49, 15.1). Additionally, gestational age, birth weight, pulmonary hypertension and postnatal steroid use for lung disease were associated with death or tracheostomy and death or longer length of stay (Table 2).
Conclusion(s): This study describes clinical outcomes of infants with severe BPD. Infants with grade 3 BPD had longer length of stay and higher need for tracheostomy. However, a considerable proportion of infants with grade 2 BPD experience death, tracheostomy and longer length of stay. These infants also have comparable rates of other adverse outcomes such as pulmonary hypertension and need for systemic corticosteroids. This data would be important in counselling families and determine timing for clinical interventions. Further studies should replicate these findings in a larger cohort of extremely preterm infants.
Table 1. Clinical characteristics and outcomes of the study cohort.
Table 2. Risk factors for death or Tracheostomy and death or longer length of stay

 photo")