604 - Reducing Routine Screening Labs for Patients in the Pediatric Emergency Department Requiring Psychiatric Admission: A Quality Improvement Initiative
Friday, April 24, 2026
5:30pm - 8:00pm ET
Publication Number: 1581.604
Jack M. Christian, Johns Hopkins University School of Medicine, Baltimore, MD, United States; Ann Marie Nolan, Johns Hopkins University School of Medicine, Baltimore, MD, United States; Sumrah Jilani, Johns Hopkins University School of Medicine, Baltimore, MD, United States; Jasmine Kung, Johns Hopkins University School of Medicine, Baltimore, MD, United States; Sarah WFFS. Edwards, University of Maryland School of Medicine, Baltimore, MD, United States; Ann Kane, Johns Hopkins School Of Medicine, Baltimore, MD, United States; Leticia Ryan, Johns Hopkins University School of Medicine, Baltimore, MD, United States; Hanae Fujii-Rios, Johns Hopkins University School of Medicine, Baltimore, MD, United States
Medical Student Johns Hopkins University School of Medicine Baltimore, Maryland, United States
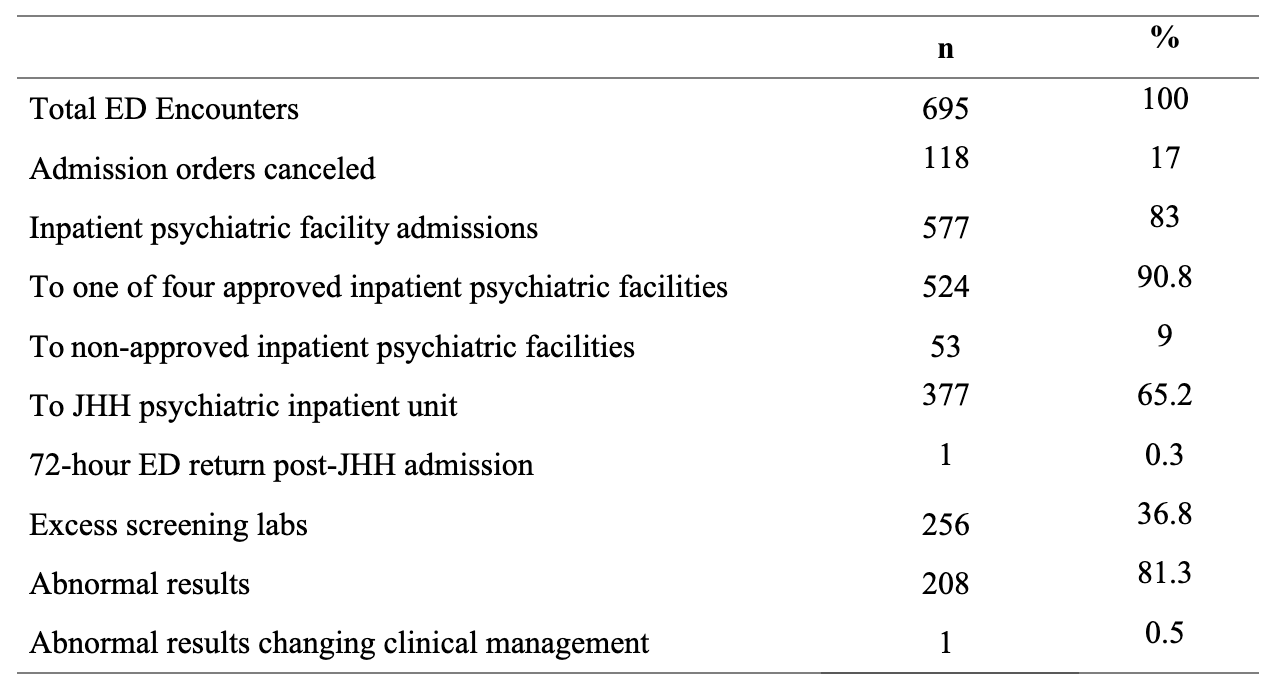
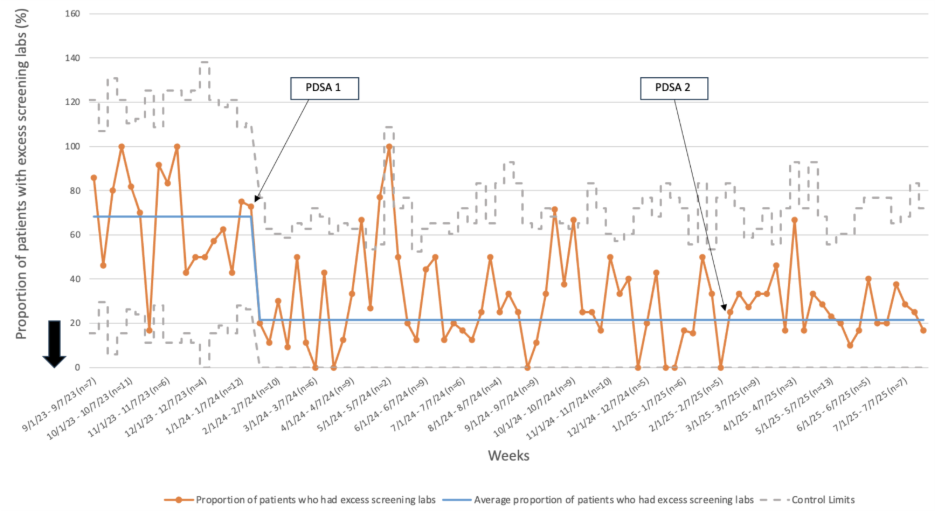
Background: Routine psychiatric admission screening labs conducted in the pediatric emergency department (ED) seldom alter medical management. Instead, they unnecessarily increase health care costs, extend ED boarding time, and cause invasive procedures for patients. National recommendations, including Choosing Wisely, advise against routine laboratory screening for pediatric psychiatric admissions unless clinically indicated. Rising pediatric mental and behavioral health ED visits and prolonged boarding times further underscore the need to de-implement low-value testing and standardize medical clearance. Objective: We aimed to reduce unnecessary routine screening labs obtained during the medical clearance process for pediatric patients requiring inpatient psychiatric admission in the ED from 68% to 20%. Design/Methods: This quality improvement initiative was conducted in an academic, urban pediatric ED. A multidisciplinary team developed a process map, fishbone diagram, Plan-Do-Study-Act cycles, and a SPC chart. Interventions included (1) partnership with four regional psychiatric facilities to minimize screening labs to urine toxicology, urine hCG, and COVID-19 testing, and (2) educational initiatives for trainees in the pediatric ED. The primary outcome was the proportion of patients receiving unnecessary screening labs. As a balancing measure, 72-hour ED returns for medical stabilization were monitored. Results: From September 1, 2023, to July 21, 2025, 695 ED encounters for mental and behavioral health conditions resulted in psychiatric admission orders (Table 2). Among 561 unique patients (mean age 14.6 ± 2.6 years), most were Black or African American (54.4%), with suicidal ideation (42.2%) and aggressive behavior (23.7%) as the leading admission diagnoses (Table 1).
Over the study period, excessive screening labs decreased from 68% to 21%, with sustained special cause variation (Figure 1). Only one patient (0.3%) required ED return for medical stabilization within 72 hours of admission, unrelated to laboratory testing (Table 2). Across all encounters, only one screening laboratory result (0.5%) led to a change in clinical management (iron initiation for iron deficiency identified on routine CBC).
Conclusion(s): Standardizing medical clearance in collaboration with psychiatric facilities and educating ED trainees resulted in a sustained reduction in unnecessary screening labs without compromising patient safety. This streamlined approach minimized invasive testing and demonstrated that routine psychiatric screening labs rarely influence clinical management.
Table 1. Pediatric ED demographics for psychiatric admission (September 2023 - July 2025) a Median (range) b "Other" includes: self-selected "other" race, American Indian or Alaska Native, Native Hawaiian or Other Pacific Islander, 2 or more races, and unknown c "Other" includes: other admission diagnosis not listed, post-traumatic stress disorder, and substance use Abbreviations: MDD, Major Depressive Disorder
Table 2. Pediatric ED to psychiatric admission and excess screening labs
Figure 1. P chart: Proportion of patients in the pediatric emergency department who have excess screening labs prior to being admitted to a psychiatric hospital

 photo")
.png) a Median (range)
a Median (range)