527 - Vasoactive drug use in children with community acquired septic shock in Australia and New Zealand
Friday, April 24, 2026
5:30pm - 8:00pm ET
Publication Number: 1506.527
Elliot Long, The Royal Children's Hospital, CLIFTON HILL, Victoria, Australia; Stephen Hearps, Murdoch Children's Research Institute, Parkville, Victoria, Australia; Amanda Williams, MCRI/RCH, Parkville, Victoria, Australia; Warwick Butt, The Royal Children's Hospital, melbourne, Victoria, Australia; Meredith L. Borland, University of Western Australia, Nedlands, Western Australia, Australia; Simon J. Erickson, Perth Children's Hospital, CLAREMONT WA 6010, Western Australia, Australia; Shefali Jani, SCHN, Castle Hill, New South Wales, Australia; Marino Festa, Children's Hospital at Westmead, Sydney, New South Wales, Australia; Eunicia Tan, The University of Auckland, Auckland, Auckland, New Zealand; Natalie Phillips, Queensland Children’s Hospital, Windsor, Queensland, Australia; Amit Kochar, Womens And Childrens Hospital, ADELAIDE, South Australia, Australia; Simon Craig, Monash University, Clayton, Victoria, Australia; stuart R. Dalziel, Starship Children's Hospital, Auckland, Auckland, New Zealand; Shane George, Griffith University, Gold Coast, Queensland, Australia; Nathan Kuppermann, Children's National Health System, Washington, DC, United States; Franz E. Babl, The Royal Children's Hospital, Melbourne, Victoria, Australia
Emergency Physician The Royal Children's Hospital CLIFTON HILL, Victoria, Australia
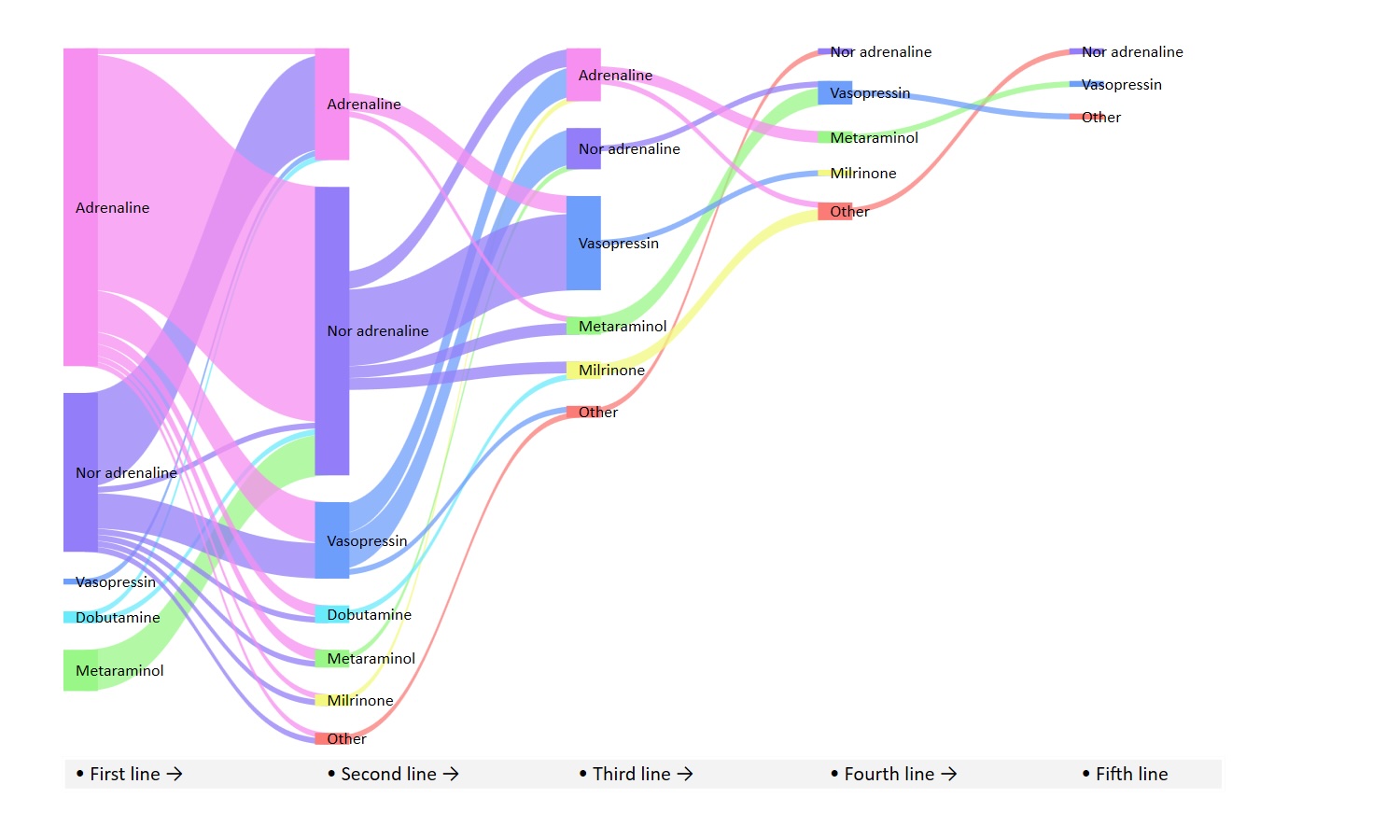
Background: Vasoactive agents are critical supportive therapies for children with septic shock. Choice and use patterns are poorly described. Objective: We describe the choice and use patterns of vasoactive agents in children with septic shock. Design/Methods: This was a prospective observational study conducted in 11 hospitals through the Paediatric Research in Emergency Departments International Collaborative (PREDICT) Network from April 2021 to December 2023. Children aged 0 to < 18 years with septic shock were included. Children admitted to the hospital and treated with parenteral antibiotics and either 1) had a provisional diagnosis of sepsis, and/or 2) were treated for suspected sepsis (fluid bolus to treat poor perfusion). The frequency and sequence of use of vasoactive agents, and contributors to the choice of initial vasoactive were collected. Results: 6232 children with septic shock were included; median age was 2.1 years (IQR 0.3-7.1 years), 60 (1.0%) died in the hospital, and 306 (4.9%) met Phoenix sepsis criteria. Vasoactive agents were used in 179 (2.9%) children overall and in 144 (45.8%) of those meeting Phoenix sepsis criteria. The most commonly used first, second, and third-line vasoactive agents were adrenaline (90/179; 50.3%), noradrenaline (49/91; 53.8%), and vasopressin (16/40; 40.0%). When comparing noradrenaline to adrenaline as first-line agents, increasing age was associated with use of noradrenaline (OR 1.12, 95% CI 1.05-1.18).
Conclusion(s): Children with suspected sepsis uncommonly received treatment with vasoactive agents. Adrenaline and noradrenaline were the most used agents, although there was substantial variation in their use and sequencing.
Table 1. Demographics, interventions and outcome in children with suspected sepsis and those requiring a vasoactive infusion. Vaso table 1.pdf
Figure 2. Choice and sequencing of vasoactive agents for the treatment of community acquired sepsis in children.
Table 3. Predictors of adrenaline vs noradrenaline as first line vasoactive for paediatric sepsis. Vaso Table 3.pdf

 photo")