Session: Neo-Perinatal Health Care Delivery: Practices and Procedures 1
710 - Prenatally diagnosis of simple VSD- to echo or not to echo?
Friday, April 24, 2026
5:30pm - 8:00pm ET
Publication Number: 1687.710
Liron Borenstein-Levin, Rambam Medical Center, Haifa, Hefa, Israel; Shiri Shifman, Technion Faculty of Medicine, Tel Aviv, Tel Aviv, Israel; Amir A. Kugelman, Rambam Medical Center, Faculty Of Medicine, Technion, Haifa, Israel, Haifa, Tel Aviv, Israel; Ori Hochwald, Rambam Medical Center, HAIFA, Hefa, Israel; Sharon Brosilow, Technion, Haifa, Israel, Ramot Menashe, HaZafon, Israel
assistant professor Rambam Medical Center Haifa, Hefa, Israel
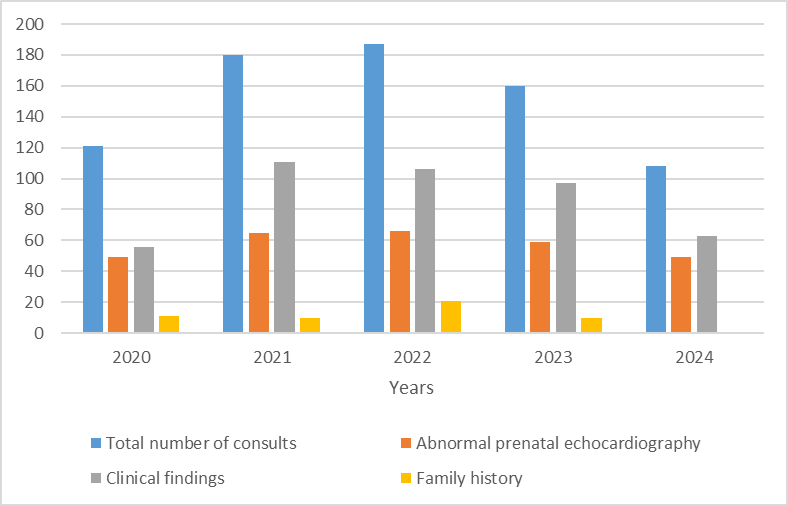
Background: Prenatal echocardiography has become increasingly common, leading to more frequent prenatal diagnoses of congenital heart defects (CHD). Among these, isolated ventricular septal defect (VSD) is the most prevalent and generally carries a favorable prognosis, often remaining asymptomatic in early life. Although VSD is not considered to have significant hemodynamic consequences in the first days of life, it is still common to refer infants for cardiology consultation after birth, and many continue to recommend delivery in tertiary centers for all prenatally diagnosed CHD cases, regardless of severity. Objective: To assess the necessity of echocardiographic evaluation during the first days of life in healthy neonates with a prenatal diagnosis or suspicion of isolated VSD. Design/Methods: Retrospective study including all infants ≥ 35 weeks' gestation admitted to the well-baby nursery at our center between January 2019 and December 2024, with a prenatal diagnosis/suspicion of isolated VSD. At our institution, neonates with abnormal fetal echocardiography routinely undergo postnatal cardiology consultation and echocardiography. We reviewed all such consultations, analyzing reasons for referral and echocardiographic findings categorized as normal, mild abnormality without hemodynamic significance, or significant abnormality with hemodynamic significance requiring early follow-up, further evaluation, or intervention. Results: Overall, 756 consultations were performed during the 5-year period (mean 151±32/year). The main reason for consultation was abnormal clinical findings- systolic murmur, tachypnea, low SpO2, or suspected syndromic features (57%), followed by abnormal prenatal echocardiography (38%). Despite improved access to care and advances in prenatal screening, the number and proportion of consults prompted by abnormal prenatal echocardiography remained unchanged. (Figure 1) Among 149 infants with prenatal suspicion of VSD, 122 (82%) were asymptomatic. 53 (36%) had normal postnatal echocardiogram, 54 (36%) had mildly abnormal findings (mostly small VSD), and only 3 (2%) had significant abnormalities (moderate-large VSDs). All three were re-evaluated within 14 days; none required medical therapy during the neonatal period.
Conclusion(s): In clinically healthy neonates, a prenatal diagnosis of isolated VSD does not appear to necessitate delivery in tertiary centers or echocardiographic evaluation in the first days of life unless clinical signs are present. This approach may safely reduce unnecessary consultations and resource utilization.
Trends in Cardiology Consultations by Year and Reason