221 - Barriers for Pediatric Injury Patients at the First Site of Care in Northern Tanzania: A Mixed Methods Study
Friday, April 24, 2026
5:30pm - 8:00pm ET
Publication Number: 1210.221
Elizabeth M. Keating, University of Utah, Salt Lake City, UT, United States; Rosalia E. Njau, Kilimanjaro Christian Medical Centre, Kilimanjaro, Kilimanjaro, Tanzania; Baraka Gipson. Moshi, KCRI, moshi, Kilimanjaro, Tanzania; Getrude M. Nkini, KCMC-Duke Collaboration, Moshi mjini, Kilimanjaro, Tanzania; Nancy Stewart. Mmary, Mwenge Catholic university, Kilimanjaro, Kilimanjaro, Tanzania; Deusdedith Evarist. Marandu, Hai Hospital, Moshi, Kilimanjaro, Tanzania; Emmanuel Benard. Minja, Hai District Hospital, Moshi, Kilimanjaro, Tanzania; Itikija Edward. Msuya, Hai District Council, Kilimanjaro, Kilimanjaro, Tanzania; Matti Koenig, University of Utah, Rootstown, OH, United States; Edwin Joseph. Shewiyo, KCMC University, Kilimanjaro, Kilimanjaro, Tanzania; Cassidy Huun, University of Utah School of Medicine, Murray, UT, United States; Sharla Rent, Duke University School of Medicine, Chapel Hill, NC, United States; Heather Keenan, University of Utah School of Medicine, Salt Lake City, UT, United States; Jennie L. Hill, University of Utah School of Medicine, Salt Lake City, UT, United States; Melissa H. Watt, University of Utah, School of Medicine, Population Health Sciences, Salt Lake City, UT, United States; Catherine Staton, Duke University School of Medicine, Durham, NC, United States; Blandina Theophil. Mmbaga, Kilimanjaro Christian Medical Centre, Moshi, Kilimanjaro, Tanzania; Joao Ricardo Nickenig Vissoci, Duke University School of Medicine, Durham, NC, United States; Joachim Magoma,Kilimanjaro Christian Medical Centre, Moshi, Tanzania; Francis Sakita, Kilimanjaro Christian Medical Centre, Moshi, Tanzania
Assistant Professor University of Utah Salt Lake City, Utah, United States
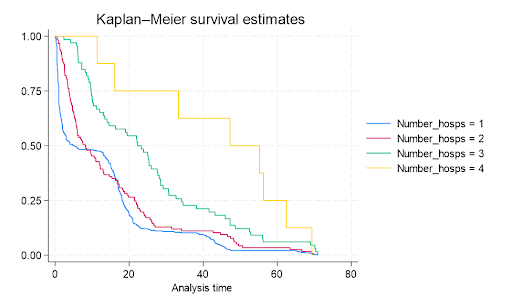
Background: Every day, 1900 children die from an injury; the majority in low- and middle-income countries. Pediatric injury patients in Tanzania face many barriers in reaching definitive care which cause delays that impact their outcomes. Objective: To identify patient, provider, and systems-level barriers for pediatric injury patients at the first site of care in order to develop an intervention to reduce the time to definitive care. Design/Methods: In this mixed methods study, we established a pediatric injury registry at three health facilities spanning the health system in Northern Tanzania. We summarized demographic and clinical characteristics using descriptive statistics. Time was defined as the median time from injury to reaching definitive care in hours. Kaplan-Meier curves were built to depict time to definitive care. We engaged 30 family caregivers of pediatric injury patients, who were referred for definitive care, in in-depth interviews. Four focus group discussions were held with healthcare providers to understand barriers when determining disposition. The Consolidated Framework for Implementation Research 2.0 framed interview guides and the thematic analysis of our qualitative data. Results: Of 784 patients enrolled in the pediatric injury registry from Aug 2024 to Sept 2025, 275 patients were referred for definitive care. Mean age was 7.2 years; 32% female. Falls, road traffic injuries, and burns were the most common injury mechanisms. The majority of patients visited one to four facilities before reaching definitive care (range 1-6) (Figure 1). Median time from injury to first health facility was 2.1 hours (0.7,18.1), time from first to second health facility was 7.6 hours (2.7,30.0), time from second to third health facility was 21.4 hours (4.7,52.5), and time from third to fourth health facility was 24.2 hours (8.0,40.3) (Figure 2). Family caregivers expressed frustration with referral delays and a need for counseling on referral decisions. Healthcare providers identified the need for more training and a decision support tool to help with referral decisions.
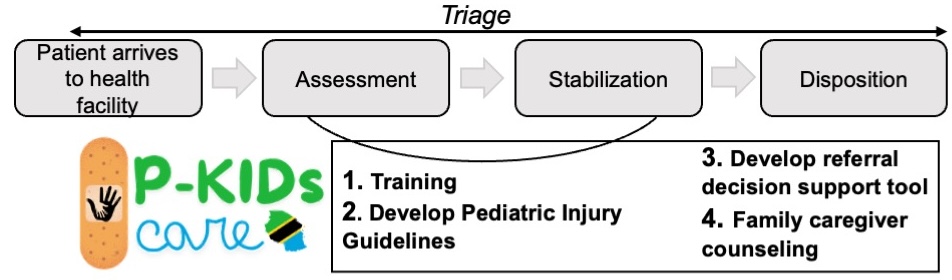
Conclusion(s): According to WHO standards, every child needing referral should be sent within 2 hours of arrival. In order to improve the referral delays found in our study, healthcare providers at the first site of care need pediatric injury care training and referral decision support. Our team will use these findings to develop and pilot a bundled intervention for pediatric injury care, P-KIDs CARE, consisting of (1) training, (2) development of guidelines, (3) a referral decision support tool, and (4) family caregiver counseling (Figure 3).
Figure 1. Survival curves showing time to definitive care for patients going from one to four health facilities before reaching definitive care.
Figure 2. Pathway to care for pediatric injury patients in our study showing median times at each health system segment.
Figure 3. Planned P-KIDs CARE intervention with four bundled components.

.jpg)