470 - Video Laryngoscopy Improves First-Attempt Intubation Success in the Delivery Room for Infants with Congenital Anomalies
Friday, April 24, 2026
5:30pm - 8:00pm ET
Publication Number: 1452.470
Gabriella Javier, Brigham and Women's Hospital, Staten Island, NY, United States; Alyssa R. Thomas, Brigham and Women's Hospital, SOUTH BOSTON, MA, United States; Margaret F. Everett, Harvard Medical School, Boston, MA, United States; Elisa Abdulhayoglu, Brigham & Women's Hospital, Lynnifeld, MA, United States
Undergraduate Student at Cornell University Brigham and Women's Hospital Staten Island, New York, United States
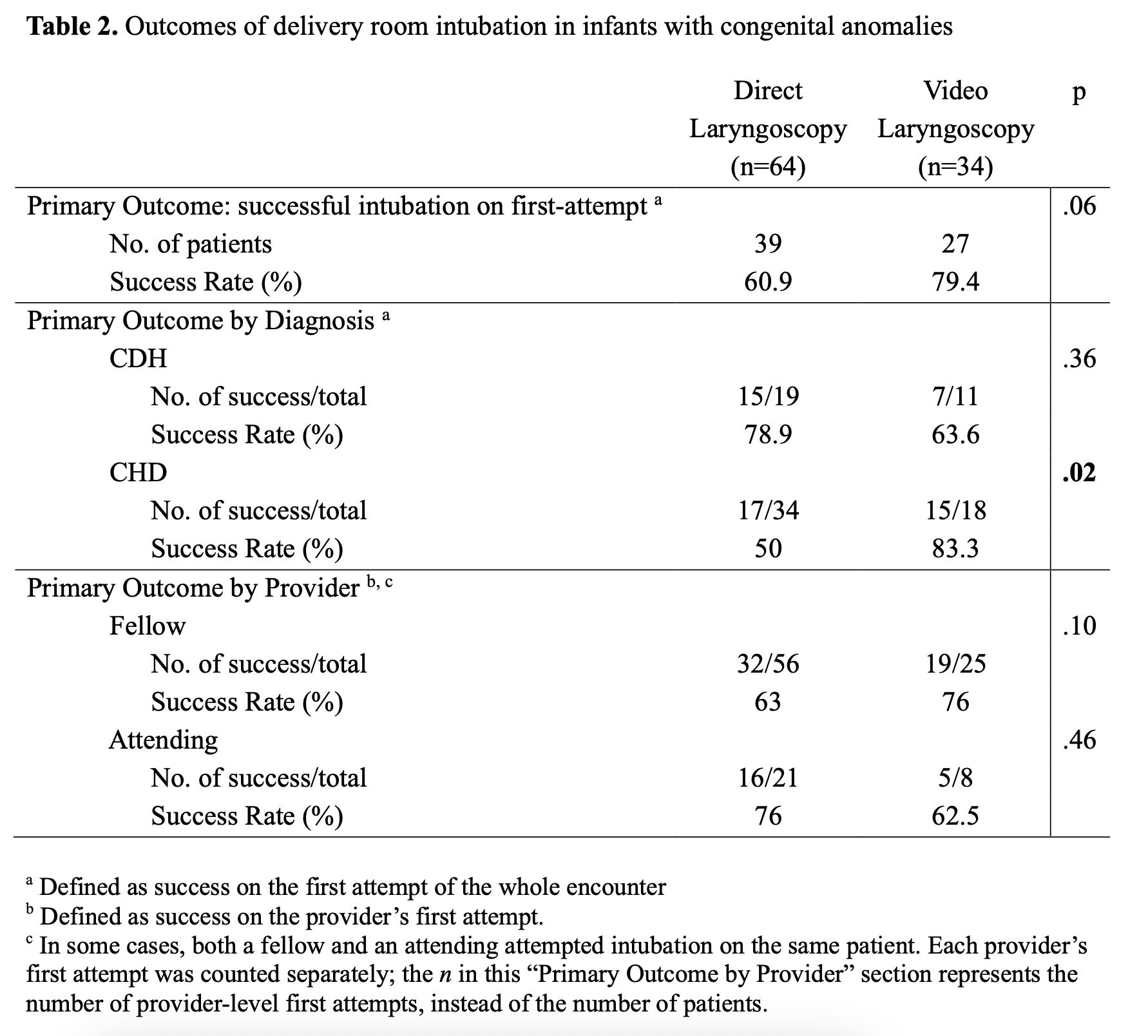
Background: Approximately 200 infants with congenital anomalies are born annually at Brigham and Women's Hospital. These infants often require immediate intubation in the delivery room (DR), where first-attempt success is critical for safe and effective resuscitation. Video laryngoscopy (VL) has been associated with improved intubation success in other neonatal settings, but its effectiveness during DR resuscitation of infants with congenital anomalies is underexplored. In September 2024, VL was implemented as the standard approach for DR intubation of newborns with congenital anomalies born at BWH. Objective: To evaluate first-attempt success when using VL versus direct laryngoscopy (DL) for DR intubation of infants with congenital anomalies, stratified by diagnosis or provider type. Design/Methods: We conducted a retrospective chart review of infants with congenital anomalies who underwent DR intubation between September 2022 and September 2025. Collected data included infant demographics, diagnosis, intubation characteristics, and number of attempts per encounter and per provider. Comparisons between VL (GlideScope®) and DL were performed using chi-square or Fisher's exact test. A run chart assessed VL adherence. This study was deemed exempt by IRB-2025P001642. Results: Ninety-eight infants with congenital anomalies were intubated in the DR, including 30 with congenital diaphragmatic hernia and 52 with congenital heart disease (CHD), the majority with transposition of the great arteries (n=36). DL was used for the first-attempt in 64 cases and VL in 34 cases. Overall, first-attempt success was higher with VL (79%) than DL (61%) (p=.06). Among infants with CHD, first-attempt success was significantly higher with VL (83%) versus DL (50%) (p=.02). Among neonatal fellows, first-attempt success was 76% for VL and 63% for DL (p=.10); among attendings, 63% for VL and DL for 76% (p=.46). On two occasions, providers reverted to DL after a failed VL attempt. The proportion of DR intubations performed with VL increased over time, reaching full adherence in May 2025.
Conclusion(s): VL improved first-attempt intubation success during DR resuscitation of infants with congenital anomalies, particularly those with CHD. These findings suggest that VL may enhance intubation performance during DR resuscitation of newborns with congenital anomalies and support its use as a first-line approach for high-risk deliveries in this population. Next steps include evaluating the association between VL use, physiological indicators of stability, and intubation duration.
Table 1. Demographic Characteristics of Infants with Congenital Anomalies Intubated in the Delivery Room
Table 2. Outcomes of delivery room intubation in infants with congenital anomalies
Figure 1. Control Chart: Percent Intubations Performed with Video Laryngoscopy

.jpg "Gabriella Javier photo")
.png)
.png)
