607 - Implementing Universal Depression Screening in Pediatric Emergency Departments
Friday, April 24, 2026
5:30pm - 8:00pm ET
Publication Number: 1584.607
Rachel Cafferty, University of Colorado School of Medicine, Aurora, CO, United States; Shaela Moen, Children's Hospital Colorado, Edgewater, CO, United States; Cortney Braund, Children's Hospital Colorado, Denver, CO, United States; Betsey Bucca, Children's Hospital Colorado, Aurora, CO, United States; Ryan Caltagirone, Children's Hospital Colorado, Denver, CO, United States; Beau Carubia, University of Colorado School of Medicine, Aurora, CO, United States; Bernadette K. Johnson, Children's Hospital Colorado, Aurora, CO, United States; David Listman, University of Colorado School of Medicine, Denver, CO, United States; Sarah Schmidt, Childrens Hospital Colorado, Aurora, CO, United States; Alexandria Wiersma, Childrens Hospital Colorado, Aurora, CO, United States
Assistant Professor University of Colorado School of Medicine Aurora, Colorado, United States
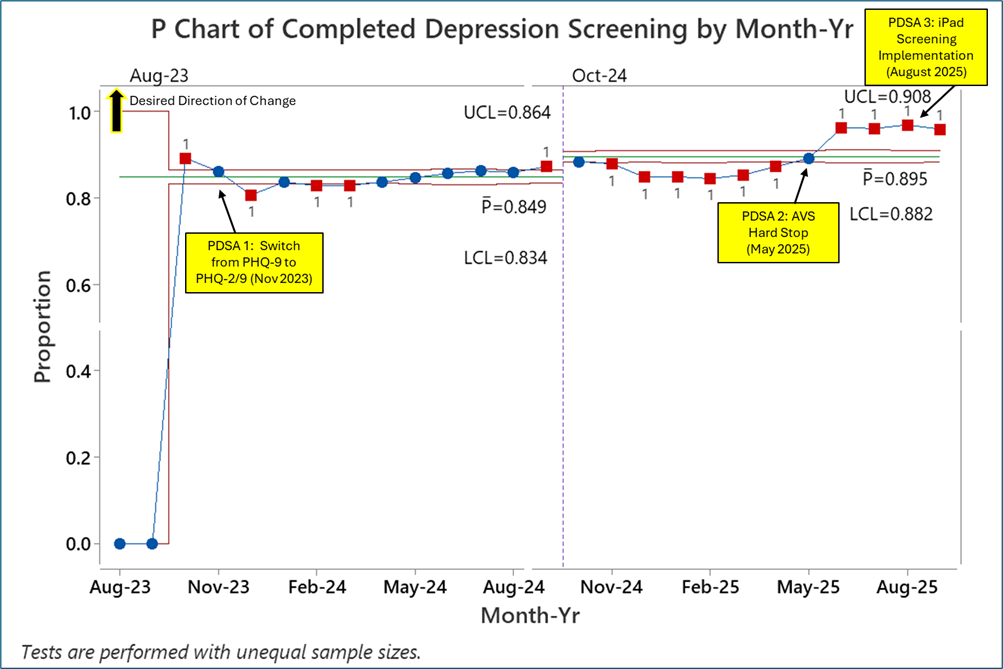
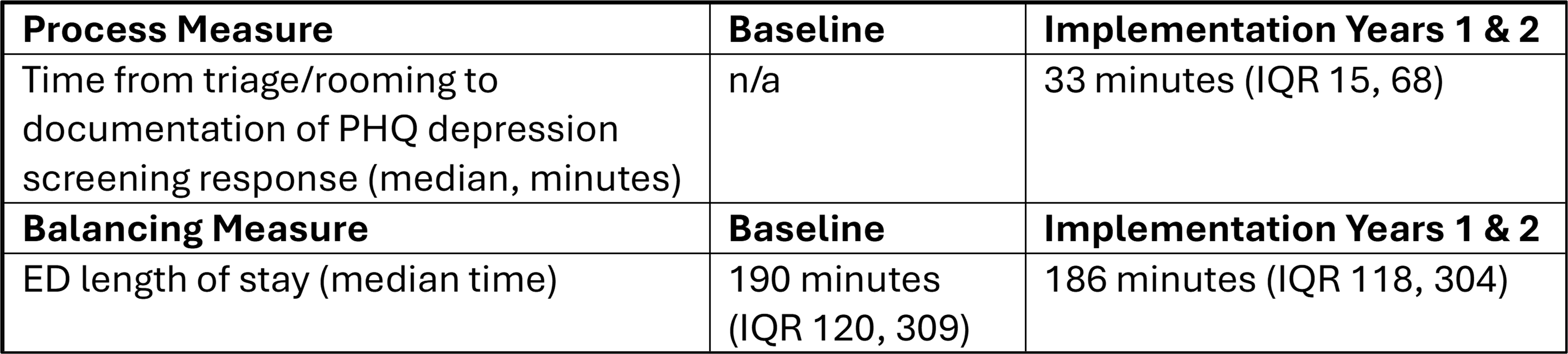
Background: In the United States, over 2.5 million youth have severe major depression; approximately half are not diagnosed until adulthood. The pediatric Emergency Department (ED) is an important healthcare touchpoint for many youths and may be an opportune setting to screen patients for symptoms of depression. In 2023, in response to the evolving pediatric mental health crisis and a state-wide initiative, Children's Hospital Colorado implemented universal depression screening in four EDs. Objective: For youth ≥10 years presenting to the ED, we will increase the proportion of eligible patients who complete universal depression screening from zero to ≥80% by September 2024 (year one), ≥85% by September 2025 (year two), and ≥90% by September 2026 (year three). Design/Methods: A multidisciplinary team applied Plan Do Study Act (PDSA) methodology to characterize current state, design project elements, and develop implementation strategies. We utilized a validated depression screening tool, the Patient Health Questionnaire (PHQ)-2/9, and included the following interventions: adapting equipment, audit and feedback, educational materials and training, clinician/staff reminders, integration in the electronic health record, and a hard stop requirement. We offered an optional brief mental health consult in the ED for patients with a moderately severe/severe PHQ score. The primary outcome measure was percentage of eligible patients who completed depression screening. Process measures included the time from triage/rooming to complete documentation of PHQ depression screen responses. Balancing measures included ED length of stay (LOS) in minutes. Results: During a two-year period, 93,129 youth (44,597 (85.28 %) in year one; 48,532 (89.88%) in year two) completed depression screening in the EDs (Figure 1). Of these, 8,168 (8.77%) screened moderately severe/severe on the PHQ-9 (3,858 year one; 4,310 year two); 426 elected to receive a brief mental health consult before ED discharge. Median time from patient rooming to documentation of PHQ-2/9 results was 33 minutes (IQR 15,68). Median total LOS during the implementation effort was 186 minutes (IQR 118, 304), compared to 190 minutes (IQR 120, 309) at baseline (Table 1).
Conclusion(s): We implemented universal depression screening for youth ≥10 years in four pediatric EDs, achieving pre-specified outcome measures during years one and two without negatively impacting LOS. This quality improvement project can provide a framework for implementation of validated pediatric mental health screening instruments across large volume, high acuity healthcare systems.
Figure 1. P chart of completed depression screening by Month-Year