581 - Identifying Strengths and Gaps in Pediatric Disaster Response: Findings from the Disaster Response Collaborative
Friday, April 24, 2026
5:30pm - 8:00pm ET
Publication Number: 1558.581
Jonathan R. Eisenberg, University of Texas at Austin Dell Medical School, Austin, TX, United States; Laura D.. Aird, University of Texas at Austin Dell Medical School, Austin, TX, United States; Julie A.. Shelton, University of Texas at Austin Dell Medical School, Weaverville, NC, United States; Brent D. Kaziny, Texas Children's Hospital, Houston, TX, United States; Katherine Remick, University of Texas at Austin Dell Medical School, Austin, TX, United States
Assistant Professor University of Texas at Austin Dell Medical School Austin, Texas, United States
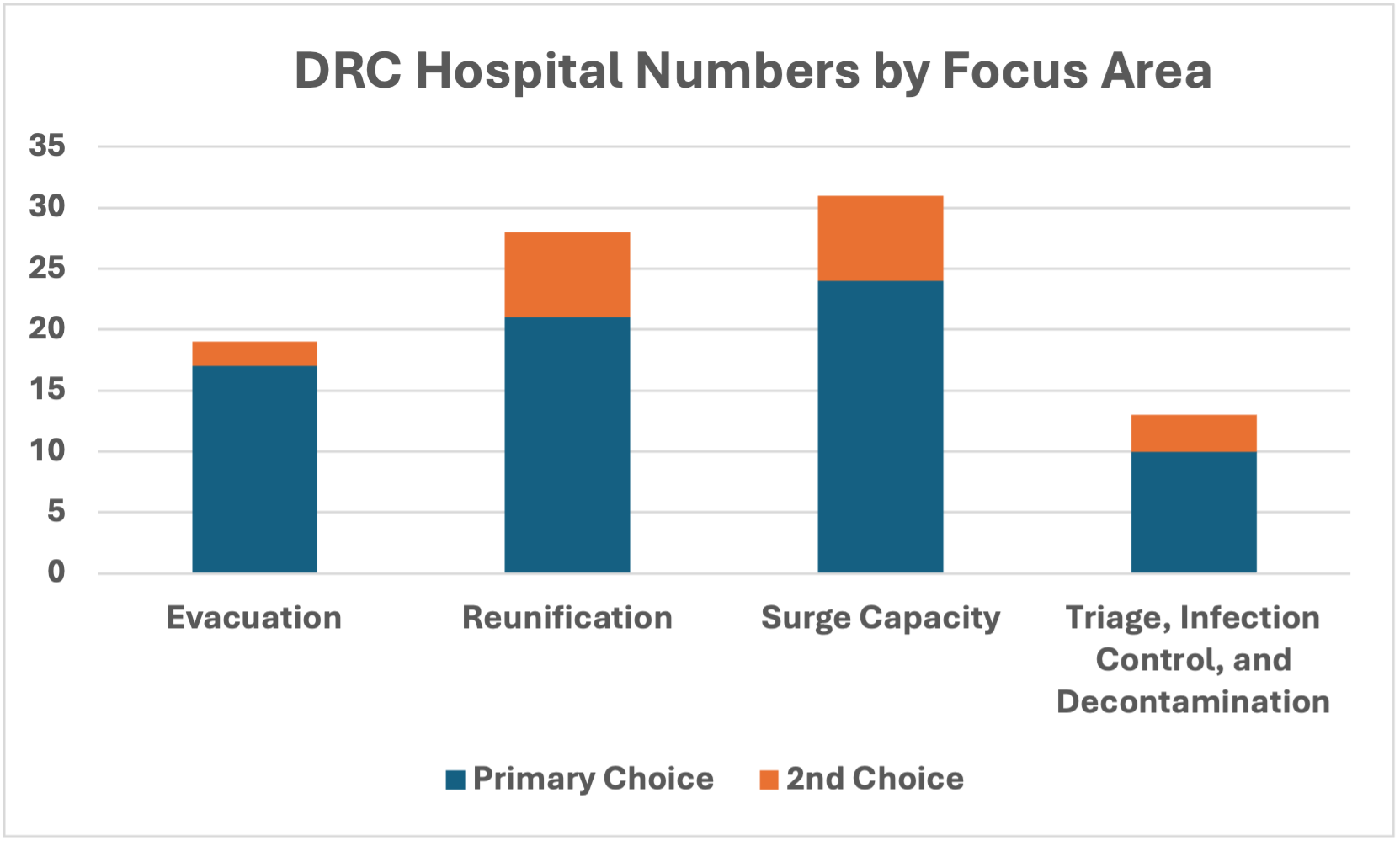
Background: The Disaster Response Collaborative (DRC) of the Pediatric Pandemic Network aims to accelerate the capabilities and capacity of children's hospitals to enhance local pediatric disaster preparedness and response (DPR). Building upon the Disaster Networking Collaborative to standardize disaster leadership roles and pediatric disaster management infrastructure, the DRC focused on improving internal and external response capabilities. Leveraging the Institute for Healthcare Improvement's Breakthrough Series Model, DRC participants engaged in self-evaluations, tabletop exercises, drills, and after-action reports to enhance pediatric disaster response. Objective: To assess strengths and weaknesses of pediatric disaster planning and response among children's hospitals during a baseline tabletop exercise. Design/Methods: Children's hospital-based disaster leadership teams were recruited to join the DRC in April 2024. Participants completed intake surveys to identify hospital characteristics and team demographics. DRC session began in September 2024. Teams selected one or more focus areas (patient tracking and family reunification, surge capacity, evacuation, and triage/infection control/decontamination) for targeted improvement efforts following six-months of orientation and learning sessions. The first tabletop drill was performed in Spring 2025 and voluntary after-action reports and action steps for improvement were collected thereafter. Results: The DRC teams represent 40 states and 1 territory with 112 children's hospitals [95 children's hospitals] participating. A total of 292 team members representing 100 hospitals completed an intake survey. Learning session attendance ranged from 146-190 attendees. Focus areas were declared by 73 hospitals (20 selected two). Tabletop exercises were completed by 54 hospitals. After-action reports were submitted by 46 hospitals, highlighting common strengths identified as activation (79%), triage (62%), and notification/communication (55%). Gaps were specific to staff training (62%), policies/written procedures (49%), and space (49%).
Conclusion(s): Children's hospitals across the U.S. are broadly engaged in collaborative efforts to improve pediatric disaster response. Identifying common strengths and vulnerabilities will help shape future improvement efforts. The DRC represents an important national step toward strengthening pediatric disaster preparedness and capacity.
Strengths and gaps identified in after action reports

 photo")
.png)