777 - Improving Outcomes of Extremely Preterm Infants Through a Small Baby Program: A Collaborative Quality Improvement Approach
Friday, April 24, 2026
5:30pm - 8:00pm ET
Publication Number: 1753.777
Miheret Yitayew, Children's Hospital of Richmond at VCU, Richmond, VA, United States; Joseph A. Khoury, Children's Hospital of Richmond at VCU, Chesterfield, VA, United States; Russell Moores, Children's Hospital of Richmond at VCU, Richmond, VA, United States; Melissa Dollings, Children's Hospital of Richmond at VCU, North Chesterfield, VA, United States; Amy H. Potter, Children’s Hospital of Richmond at VCU, New Kent, VA, United States; Lisa F. Shaver, Children's Hospital of Richmond at VCU, Glen Allen, VA, United States; Edward Henry. Springel, Virginia Commonwealth University School of Medicine, Richmond, VA, United States; Karen D.. Hendricks-Muñoz, Children's Hospital of Richmond at VCU, Richmond, VA, United States
Assistant Professor Children's Hospital of Richmond at VCU Richmond, Virginia, United States
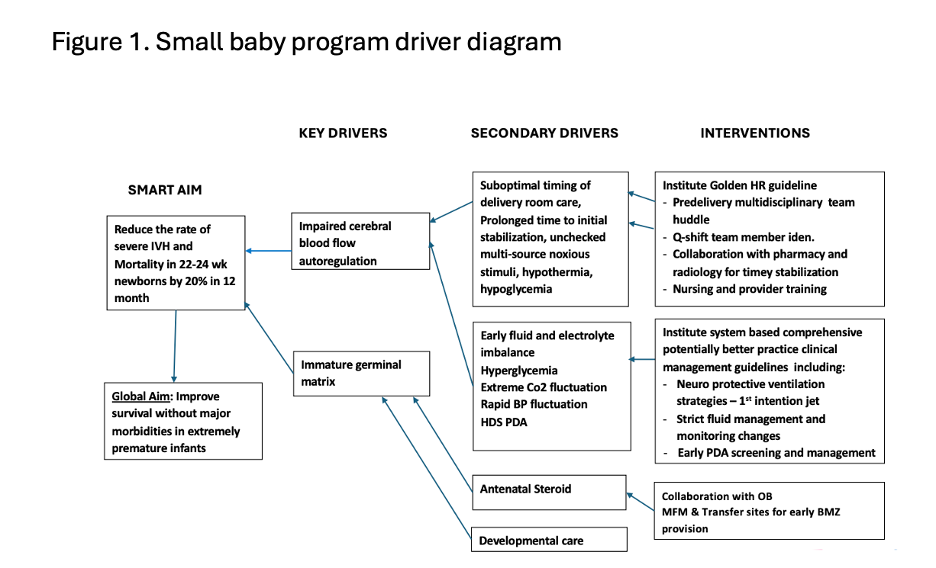
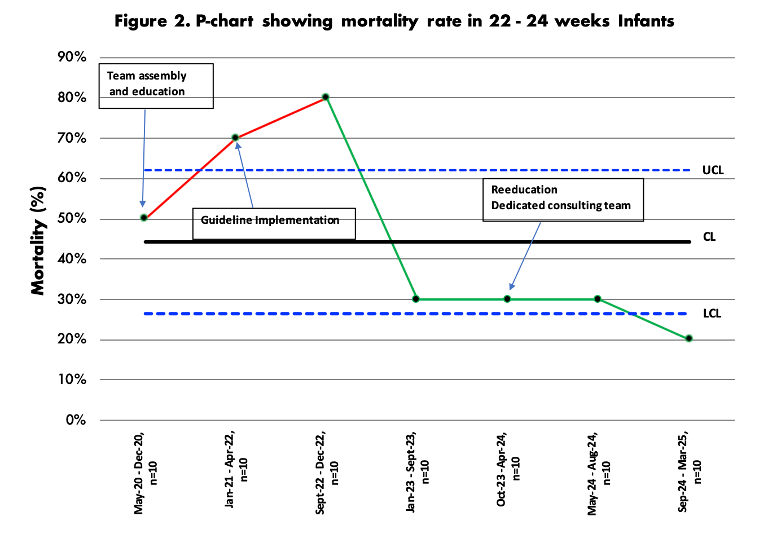
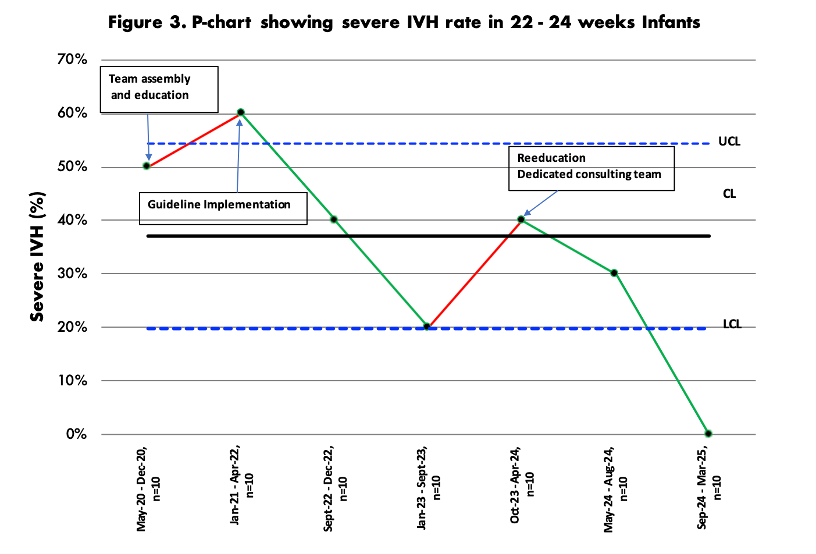
Background: Despite significant advances in neonatal care for infants born at 22 weeks gestational age (GA), these extremely preterm (ePT) infants remain at highest risk of mortality and severe morbidity. Establishment of focused small baby programs with dedicated resources, interdisciplinary care teams and standardized guidelines has been linked to improved health outcome. Our level IV regional neonatal intensive care unit implemented a multidisciplinary collaborative small baby program to improve survival and neurodevelopmental outcomes of ePT infants born at 22 week and further optimize that of infants born at 23-24 weeks gestation. Objective: To reduce mortality and intraventricular hemorrhage (IVH) in ePT infants born at 22-24-weeks GA. Design/Methods: A multidisciplinary team of NICU neonatologists, nurses, therapists, maternal fetal medicine experts, pediatric cardiologists and NICU leadership established a small baby program. Interventional phases were focused on culture, education, visits to centers with small baby programs, equipment requirements for care, integrated obstetrical care of timely maternal transfer, antenatal steroid provision, multidisciplinary pre-delivery huddle, consistent pre-delivery family counseling, as well as system based clinical and nursing standardized care guidelines. Mortality and IVH pre- and post-intervention (May 2020-Aug 2022) and (Sept 2022- Mar 2025) respectively were analyzed for all inborn ePT infants admitted to the NICU. Pareto charts and driver diagram were used to identify areas of focus for intervention, Figure 1. Statistical process run charts were done to assess impact in primary outcome overtime after every 10-newborn cohort. Results: A total of 70 inborn infants , 30 from pre- and 40 from post-intervention period were analyzed. Median GA and birthweight were not different in both periods. Mortality declined across gestational age (50% to 20%) with an improvement in survival to discharge in 22week gestation infants from 22% to 71%, p=0.04 . Infants with severe IVH declined overtime from 50% to 0% following intervention in all gestational age categories, Figure 2 & 3.
Conclusion(s): Unique challenges and controversies surround the care of ePT infants born at 22-24 weeks. Development of a focused small baby program with institutional investment, stakeholder by-in, interdisciplinary education and family centered interprofessional collaboration can improve survival and short-term morbidity outcomes of these most vulnerable newborns.

 Credit")