44 - NeoCH Score: Classification of Intracranial Hemorrhage Secondary to Neonatal Cerebral Venous Sinus Thrombosis
Friday, April 24, 2026
5:30pm - 8:00pm ET
Publication Number: 1037.44
Rhandi Christensen, The Hospital for Sick Children, Toronto, ON, Canada; Linda S. de Vries, LUMC, Leiden, Zuid-Holland, Netherlands; Mehmet Cizmeci, The Hospital for Sick Children, Toronto, ON, Canada; Pradeep Krishnan, The Hospital for Sick Children, Toronto, ON, Canada; Vann Chau, The Hospital for Sick Children, Toronto, ON, Canada; Nomazulu Dlamini, The Hospital for Sick Children, Toronto, ON, Canada; Elizabeth Pulcine, The Hospital for Sick Children, TORONTO, ON, Canada; Mahendra Moharir, The Hospital for Sick Children, Toronto, ON, Canada
Pediatric Neurologist The Hospital for Sick Children Toronto, Ontario, Canada
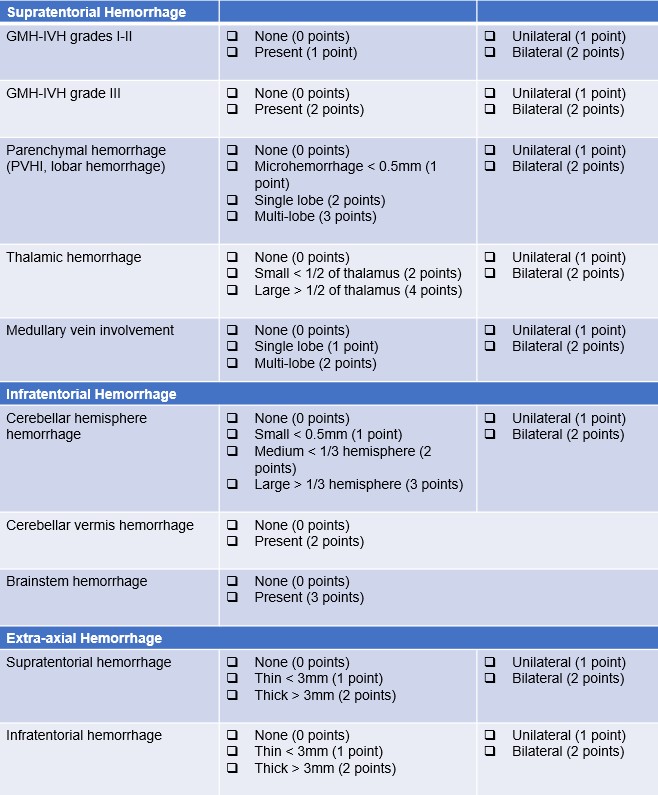
Background: Neonatal cerebral venous sinus thrombosis (CVST) often co-occurs with intracranial hemorrhage (ICH) and is associated with adverse neurodevelopmental outcomes. There is no rating scale to characterize ICH secondary to neonatal CVST. Objective: To develop the Neonatal CVST Hemorrhage Score (NeoCH Score) to classify and grade the severity of ICH in neonates with CVST. Design/Methods: This retrospective cohort study included neonates with CVST diagnosed with brain MRI/MRV. The NeoCH Score was developed using the study sample, integrating elements from previous hemorrhage classification systems and expert consensus (Figure 1). Ordinal logistic regression was used to examine the associations between NeoCH total score, stratified score (score ≥16), and subscores with neurodevelopmental outcome at the last clinic visit. All models were adjusted for prematurity, congenital heart disease, infection, ischemic brain lesions and multifocal hemorrhage. Interrater reliability was assessed with intraclass correlation coefficient. Results: The study included 100 neonates (77% term and 23% preterm) with CVST and varying degrees of ICH (Figure 2). Thrombosis of multiple venous sinuses was present in 62%. Ischemic brain lesions were present in 64% and venous infarcts in 44% (Figure 3). Supratentorial hemorrhage was present in 57%, infratentorial hemorrhage in 19%, and extra-axial hemorrhage in 32%. Most were treated with anticoagulation (66%), and 89% had partial or full thrombus recanalization. Neurodevelopmental outcomes included 36% with normal outcomes, 16% with mild impairment, 21% with moderate impairment, and 17% with severe impairment. NeoCH subscores for germinal-matrix/intraventricular hemorrhage (GMH-IVH) grade 3 (OR=3.9, P=0.009), GMH-IVH grade 3 laterality (OR=2.1, P=0.01), parenchymal hemorrhage (OR=1.7, P=0.01), parenchymal hemorrhage laterality (OR=2.2, P=0.02), and thalamic hemorrhage (OR=1.5, P=0.04) were predictors of outcomes in multivariable logistic regression. NeoCH score ≥16 was associated with worse outcomes (OR=3.9, P=0.04). Inter-rater reliability showed good agreement between reviewers with an intraclass correlation coefficient of 0.71.
Conclusion(s): The NeoCH Score is a simple clinical tool to characterize ICH secondary to neonatal CVST. Increasing NeoCH total score, GMH-IVH grade 3, parenchymal and thalamic hemorrhage subscores were associated with worse neurodevelopmental outcomes. NeoCH Score can be used clinically for risk stratification and for research purposes.