756 - Increasing the Rate of Timely Discharges in the Neonatal Intensive Care Unit
Friday, April 24, 2026
5:30pm - 8:00pm ET
Publication Number: 1732.756
Michael R. McFayden, Brody School of Medicine at East Carolina University, Winterville, NC, United States; Lindsey N. Gieselman, James and Connie Maynard Children's Hospital at ECU Health, Kinston, NC, United States; Kayla Ausbon, Brody School of Medicine at East Carolina University, Washington, NC, United States; Leeza Jones, ECU Health Medical Center, 3672 E Wilson Street, NC, United States; Uduak Akpan, Brody School of Medicine at East Carolina University, Greenville,NC, NC, United States; Mary Iwaszewski, Brody School of Medicine at East Carolina University, Greenville, NC, United States
Medical Student Brody School of Medicine at East Carolina University Winterville, North Carolina, United States
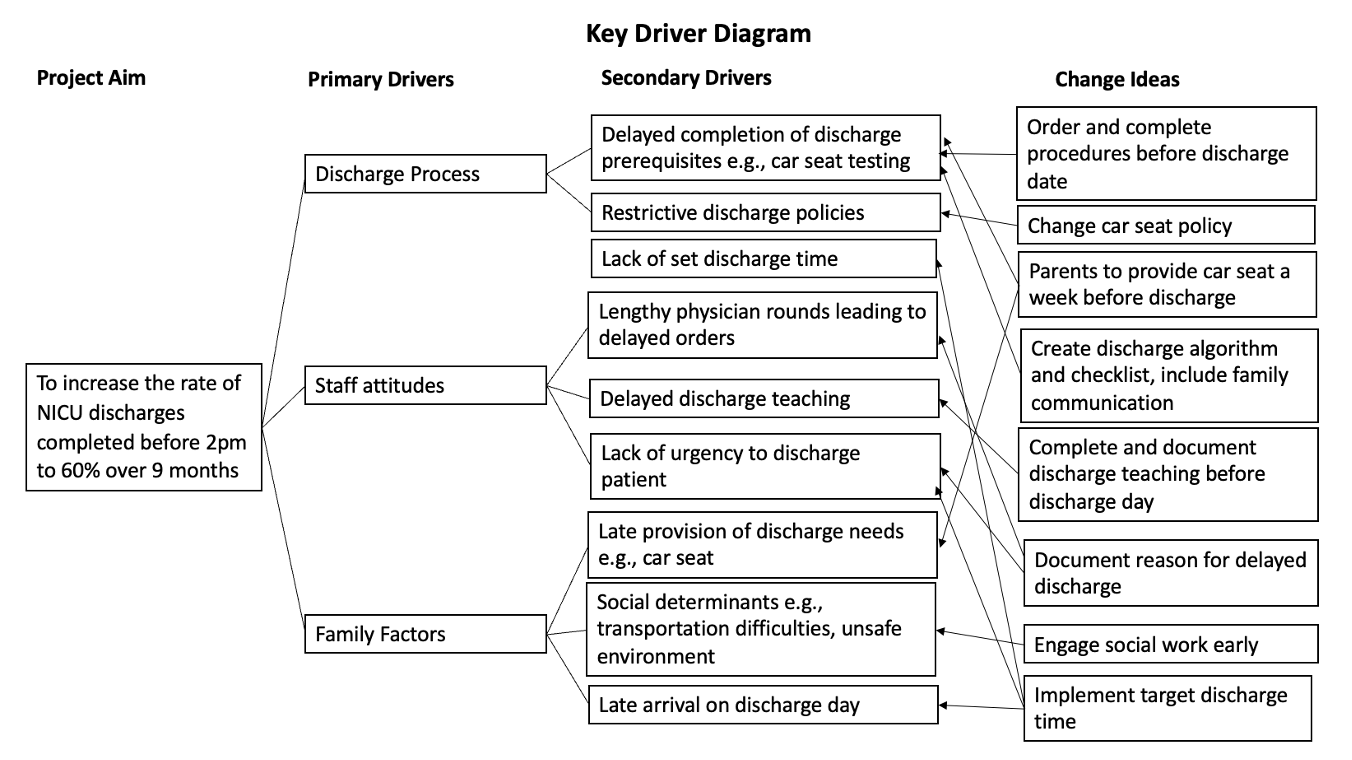
Background: Hospital discharge times have implications for resource utilization and family satisfaction. The Neonatal Intensive Care Unit (NICU) at ECU Health is a 71-bed level IV unit that admits approximately 1,000 neonates annually. Only 40% of discharges were completed before 2pm in our NICU. Therefore, to ensure efficient throughput, we implemented a Quality Improvement project to achieve earlier discharge times in the NICU. Objective: To increase the rate of NICU discharges completed by 2 PM to 60%, within 9 months. Design/Methods: We formed a multidisciplinary team and organized discharge barriers into a Key Driver Diagram. We collected baseline data and implemented a series of interventions over five Plan-Do-Study-Act (PDSA) cycles. Key interventions included establishing a NICU discharge time (PDSA 1, April 2024), amending the car seat testing policy (PDSA 2, May 2024), implementing a discharge algorithm (PDSA 3, August 2024), creating a bedside discharge checklist (PDSA 4, February 2025), and implementing order entry during morning rounds (PDSA 5, May 2025). We tracked measures using statistical process control charts and analyzed data in 2-week cycles.
Outcome Measures: Percentage of discharges completed by 2PM. Percentage of discharges completed within two hours of discharge order placement.
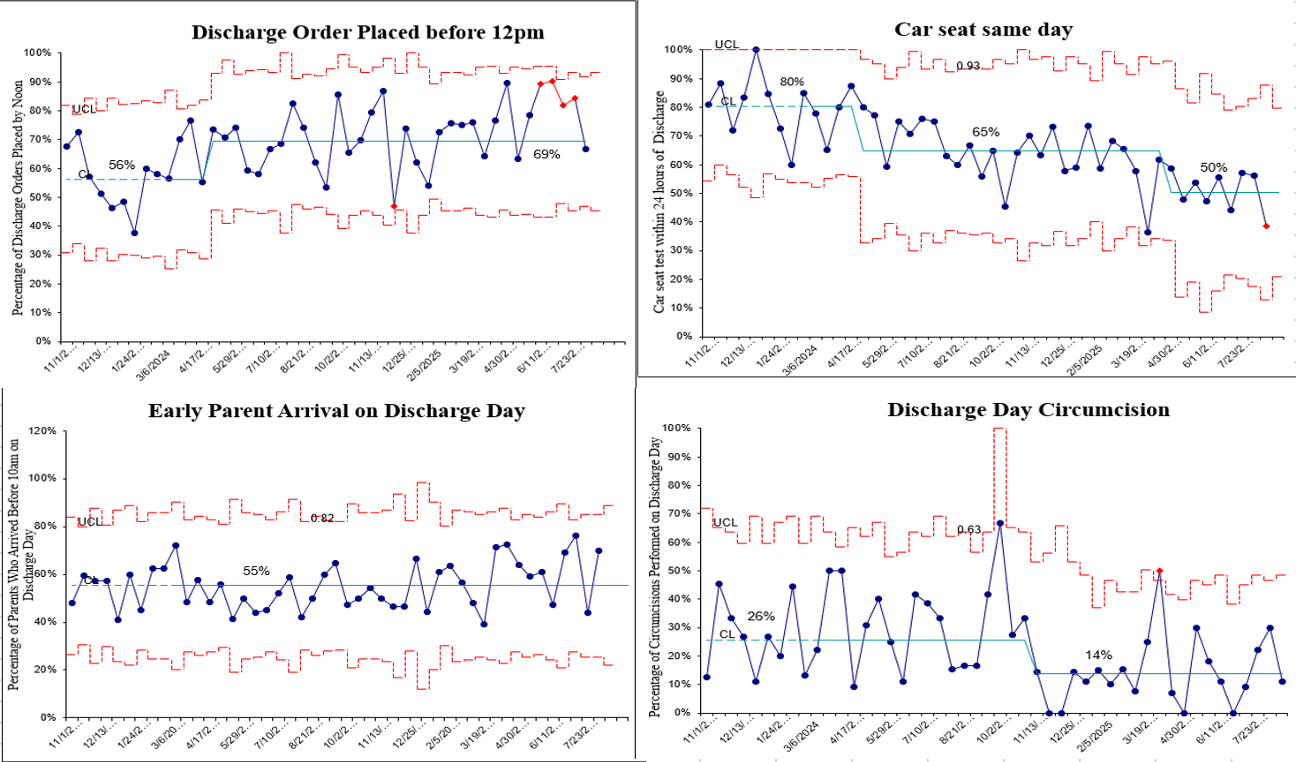
Process Measures: Percentage of discharge orders entered by noon. Percentage of parents arriving before 10 AM on discharge day. Percentage of car seat testing completed within 24 hours of discharge. Percentage of circumcisions completed on day of discharge.
Balancing Measures: Percentage of families reporting low satisfaction with discharge process. Results: We collected baseline data over 5 months for ten data cycles, and intervention data and sustainment data over 18 months. We achieved our primary aim of increasing discharges completed by 2pm to 60% and increased the rate of discharges occurring within two hours of the discharge order by 30%. Discharge order entry by noon increased by 23% while car seat testing within 24 hours of discharge and circumcisions on discharge day decreased by 38% and 46%, respectively. Parent arrival time before 10AM on discharge day and our balancing measure of parent satisfaction with the discharge process both remained unchanged throughout the project, at 55% and 85%, respectively.
Conclusion(s): We achieved our goal of earlier discharge times by integrating new or modified discharge processes into the standard NICU workflow. Socio-economic factors and inaccurate documentation contributed to unchanged parental arrival times on discharge day.

 Credit")
 photo")