56 - Disparities in NICU and Post-Discharge Outcomes in Neonates Treated with Therapeutic Hypothermia for Hypoxic-Ischemic Encephalopathy
Friday, April 24, 2026
5:30pm - 8:00pm ET
Publication Number: 1049.56
Yasmin Minai, Rush Medical College of Rush University Medical Center, Chicago, IL, United States; Kousiki Patra, Rush Medical College of Rush University Medical Center, Chicago, IL, United States
Medical Student Rush Medical College of Rush University Medical Center Chicago, Illinois, United States
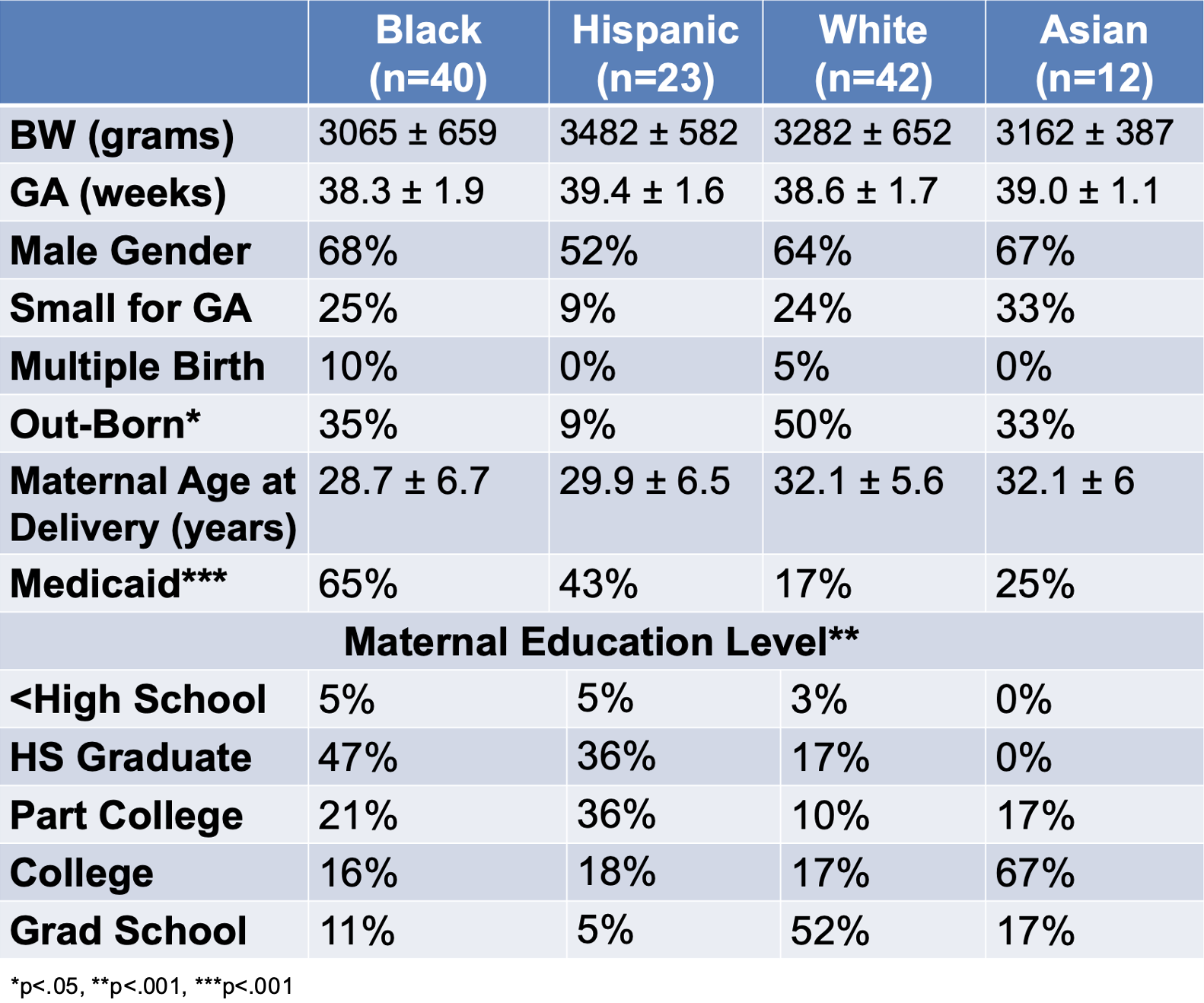
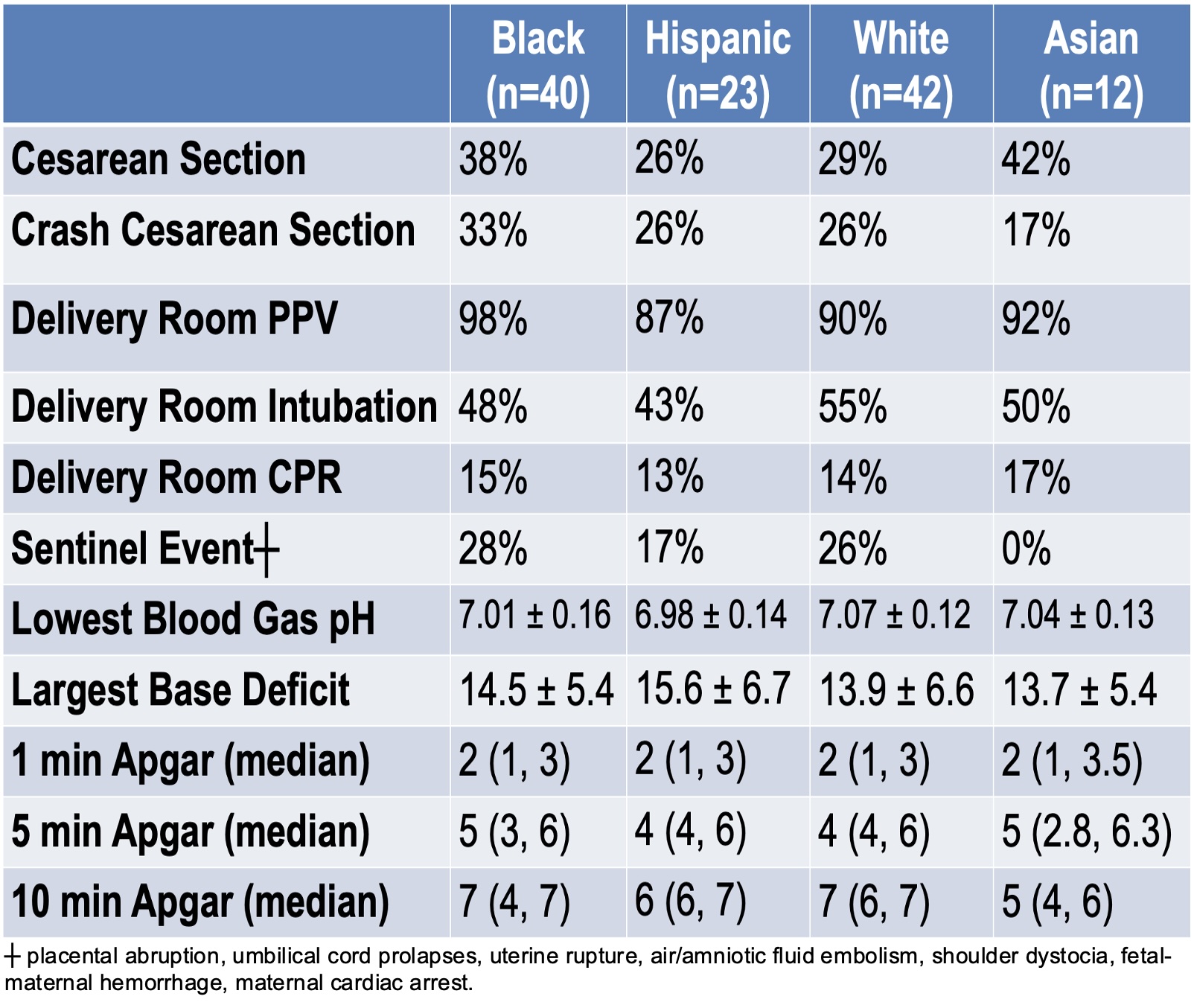
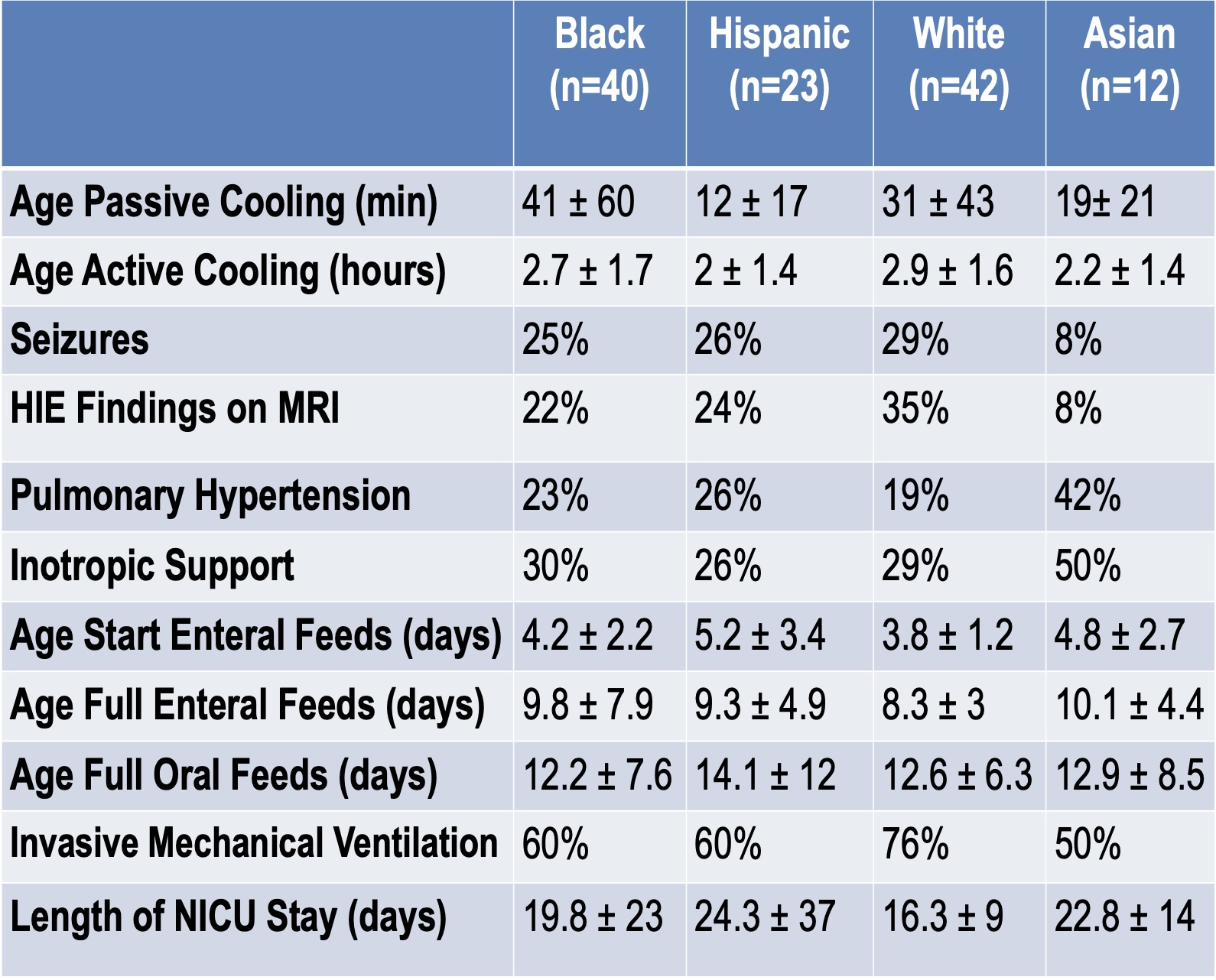
Background: Neonatal hypoxic-ischemic encephalopathy (HIE) is a significant cause of mortality, developmental delay, and adverse neurodevelopmental (ND) outcomes. Therapeutic hypothermia (TH) is the only proven therapy. Studies have shown that Black and/or Hispanic infants are less likely to be offered TH. Racial/ethnic disparities in HIE therapy and outcomes remain understudied. Objective: To examine the relationship between race/ethnicity in infants treated with TH for HIE and 1. Neonatal outcomes in the NICU and 2. Neurodevelopmental outcome at 20 months corrected age (CA). Design/Methods: This is a retrospective chart review of infants treated with TH for HIE (2017-2023), stratified by race/ethnicity into four groups: Black (B), Hispanic White (H), Non-Hispanic White (W), and Asian (A). NICU outcomes included data on socio-demographics, delivery, TH, NICU care and morbidities. ND Outcome measures included cognitive, language, and motor index scores on the Bayley Scales at 20 months CA. Similarities in maternal age, education, and insurance led to merging groups as Black/Hispanic (B/H) and White/Asian (W/A) for linear regression analyses to examine impact of race/ethnicity on ND outcome. Results: The social/birth data for the 117 infants is shown in Table 1. Mothers in the W/A group had higher education level and private insurance. No significant differences were seen among the four groups with respect to delivery, resuscitation measures or NICU outcomes (Tables 2 and 3). Racial/ethnic groups were combined due to similarities in significantly higher maternal age (p=.01), education levels (p <.001) and private insurance (p <.001) in the W/A group. Infants in the W/A group had a higher rate of out-born deliveries (p=0.03) and higher blood pH (p=0.02) compared to the B/H group. Racial/ethnic groups weren't significantly linked to ND outcomes; only seizures were associated with lower motor scores at 20 M CA (p=.037).
Conclusion(s): No significant racial/ethnic differences were found in resuscitation measures, TH timing, NICU care or outcomes. Although W/A infants had higher cognitive and language scores at 20 months CA compared to B/H infants in unadjusted analyses, these findings didn't persist after adjusting for covariates. We speculate that sociodemographic factors after NICU discharge more strongly impact cognitive and language outcomes. Future research should target post-NICU interventions to reduce social and racial inequities in children with HIE.