Session: Health Equity/Social Determinants of Health 1
181 - Association of Socioeconomic Status with Protective and Risk Practices for Sleep-Related Infant Death
Friday, April 24, 2026
5:30pm - 8:00pm ET
Publication Number: 1170.181
Isha Bhangui, University of Virginia School of Medicine, Charlottesville, VA, United States; Isabella Zaniletti, IZ Statistics LLC, Tampa, FL, United States; Jeffrey D. Colvin, Children's Mercy Hospitals and Clinics, Kansas City, MO, United States; Carolyn Ahlers-Schmidt, KUSM-W CRIBS, Wichita, KS, United States; Vicki Collie-Akers, University of Kansas School of Medicine, Kansas City, KS, United States; Christy Schunn, Kansas Infant Death and SIDS Network, Wichita, KS, United States; Rosemary Nabaweesi, Meharry Medical College, Nashville, TN, United States; Rachel Moon, University of Virginia School of Medicine, Charlottesville, VA, United States
Medical Student University of Virginia School of Medicine Broadlands, Virginia, United States
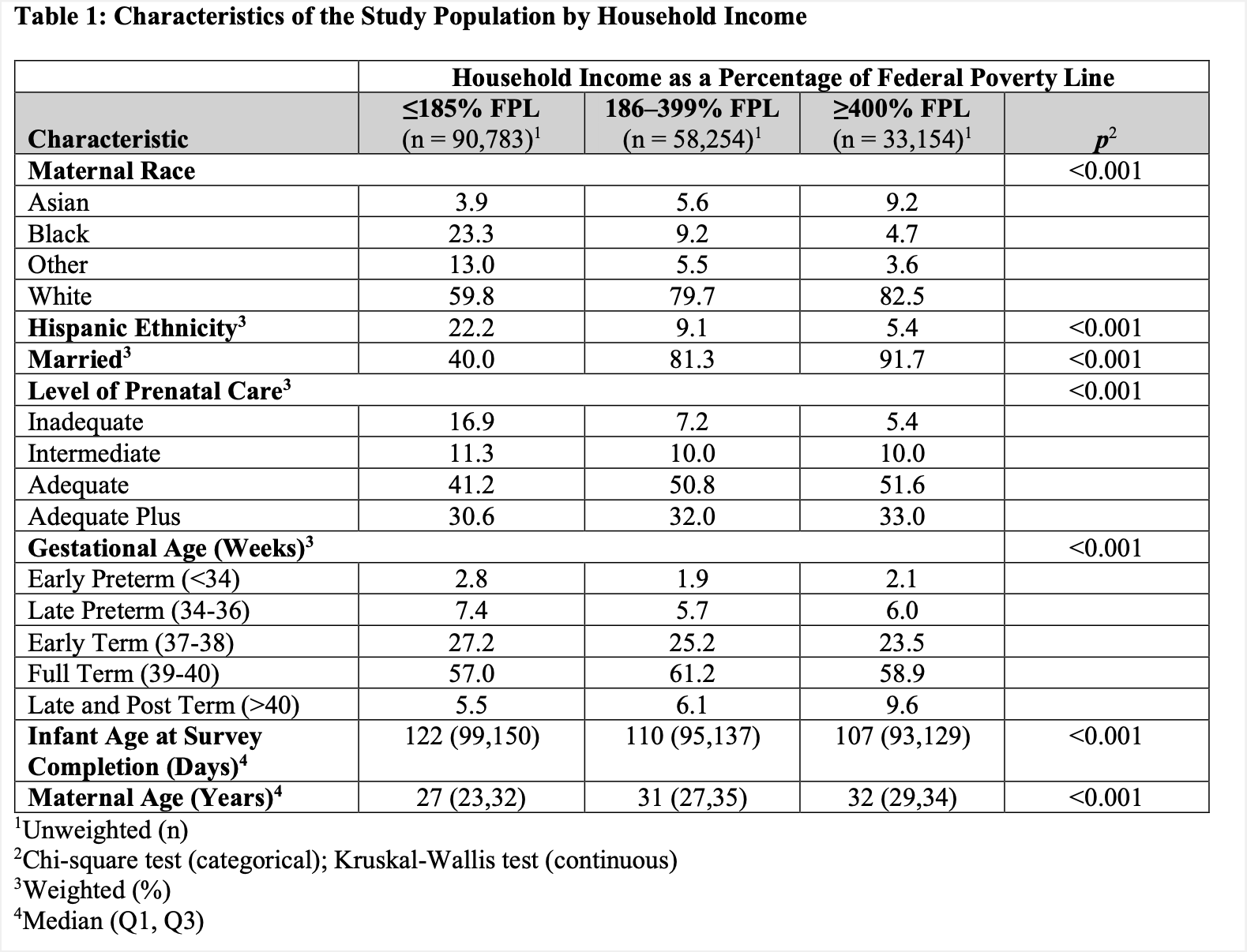
Background: Rates of sleep-related infant death among low-income households far exceed those of high-income households. To reduce the risk of sleep-related infant death, the AAP recommends key protective practices including supine sleep, safe sleep surface use, room sharing without bedsharing, and breastfeeding ≥ 8 weeks, while discouraging maternal smoking, soft or loose bedding, and more recently, e-cigarette use. Sleep sacks are recommended over loose bedding. However, little is known about how these practices vary by household income. Furthermore, potential differences in sleep sack use and maternal e-cigarette use by household income have not been previously examined. Objective: To identify whether household income is associated with specific risk and protective practices for sleep-related infant death. Design/Methods: We conducted a cross-sectional analysis of the CDC's Pregnancy Risk Assessment Monitoring System (PRAMS) data from 2016-2022. PRAMS is a sample of mothers of infants from 39 states. Our main exposure was household income as a percentage of the federal poverty level (FPL), and categorized as ≤185% FPL, 186-399%, and ≥ 400% FPL. Outcomes reflected AAP-recommended protective practices (supine sleep position, sleeping alone, use of a safe sleep surface, room sharing, sleep sack use, breastfeeding ≥ 8 weeks) and risky behaviors (soft bedding, maternal tobacco and e-cigarette use). Associations between household income and these outcomes were examined using multivariable logistic regression, adjusting for infant and maternal age, maternal race and ethnicity, marital status, prenatal care, and gestational age. Results: Characteristics of the 9.5 million weighted respondents are provided in Table 1. Infants from low-income households (≤185% FPL) had 62% lower odds of supine sleep, 40% lower odds of sleeping separately, 30% lower odds of a safe sleep surface, 69% lower odds of sleep sack use, and 54% lower odds of breastfeeding ≥8 weeks compared to high-income families (≥ 400% FPL) (Table 2). Mothers from low-income households had 159% higher odds of using soft bedding, 472% higher odds of prenatal e-cigarette use, and 1280% higher odds of cigarette smoking during pregnancy.
Conclusion(s): Current efforts to reduce sleep-related infant deaths have prioritized safe sleep. Our findings suggest enhanced support for smoking and e-cigarette cessation, sleep sack use, and lactation assistance, alongside safe sleep promotion, may be critical in reducing disparities in sleep-related infant death. Future research to understand differences by income in risk factors for sleep-related infant death is needed.
Table 1: Characteristics of the Study Population by Household Income
Table 2: Unadjusted and Adjusted Associations of Household Income with Study Outcomes

 photo")
.png)
