515 - Risk of Intussusception Associated with Gastrojejunostomy Tubes in Children with Medical Complexity: A Retrospective Cohort Study
Friday, April 24, 2026
5:30pm - 8:00pm ET
Publication Number: 1495.515
Akhila Shapiro, Children's Hospital of Philadelphia, Philadelphia, PA, United States; Ao (Sophia) Tan, Childrens Hospital of Philadelphia, Lansdale, PA, United States; Annique K. Hogan, Childrens Hospital of Philadelphia, Philadelphia, PA, United States; Chris Feudtner, Children's Hospital of Philadelphia, Philadelpia, PA, United States; Morgan Congdon, Childrens Hospital of Philadelphia, Philadelphia, PA, United States
Clinical Assistant Professor of Pediatrics Children's Hospital of Philadelphia Philadelphia, Pennsylvania, United States
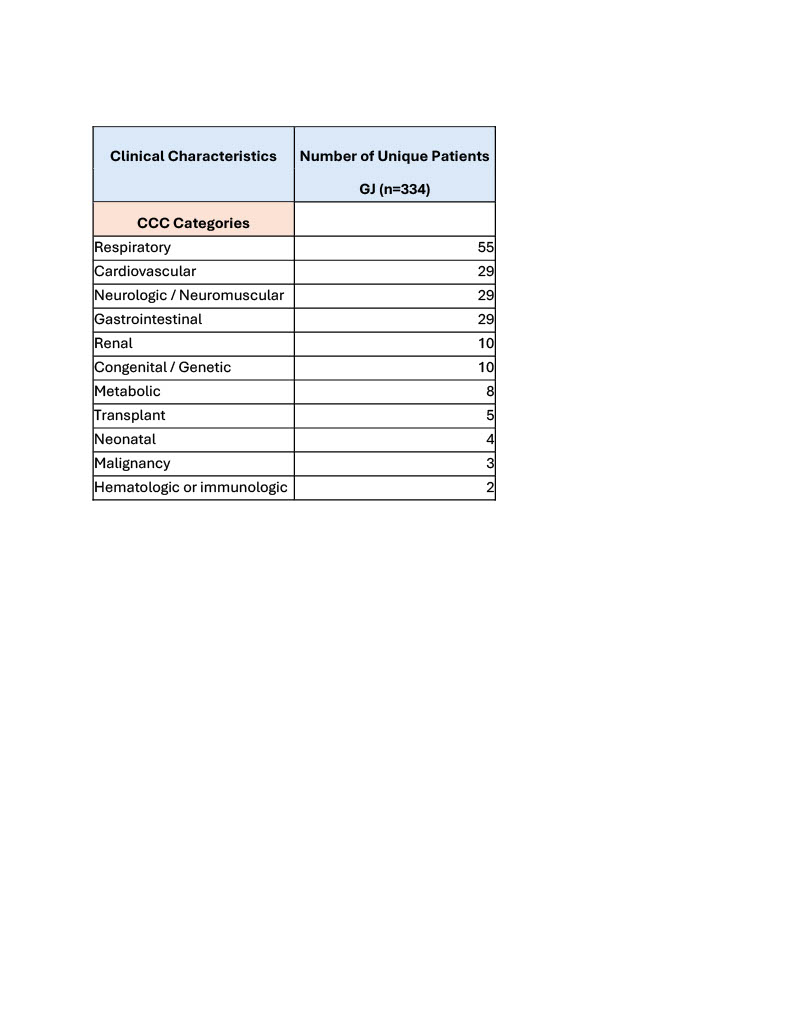
Background: Intussusception is a known complication in patients with gastrojejunostomy tubes (GJT) that can occur any time and sometimes repeatedly, often causing pain and feed intolerance. The frequency of intussusception is unknown, leading to uncertainty when weighing the risks and benefits of initial or repeat GJT placement with families. Objective: This retrospective cohort study identifies the rate of intussusception in patients with GJT over a 5 year period at a single institution and describes the risk of repeated intussusception after the initial episode. Design/Methods: We included patients from May 1, 2019 - May 31, 2024. Patients were selected for inclusion via the electronic health record using International Classification of Diseases (ICD)-9 and -10 codes: Intussusception (ICD-10 code K56.1) and GJT (ICD-10 code Z93.4) on problem lists. Demographic data including median age with interquartile range (IQR), sex, median weight with IQR, and underlying diagnoses were recorded. Pediatric Complex Chronic Conditions (CCC) were identified for the cohort. Data were analyzed using Stata and categorized according to the Pediatric Complex Chronic Condition (CCC) System Version 3. Results: A total of 334 patients met inclusion criteria. The cohort included182 male patients (54.5%), median age was 4.3 years (IQR 1.1-11.5) and median weight was 15.4kg (IQR 8.8-33.7). Eleven CCC categories were described; respiratory diagnoses were the most common category in our cohort. Thirty-nine of 334 patients experienced symptomatic intussusception along their GJT, indicating an initial rate of intussusception of 11.6%. The method of enteral nutrition was changed for 11 patients after the first episode of intussusception. Fifteen of the remaining 28 patients (53.6%) who continued with a GJT had repeated intussusception events. When the GJT remained as the feeding tube after the first intussusception event, the risk of recurrence increased progressively. At the time of last follow-up, 16 patients (41%) still had a GJT in place, and 14 patients (36%) had successfully returned to GT.
Conclusion(s): GJTs are increasingly a viable option in CMC with severe GER and risk of aspiration, but there is limited evidence on the complication of intussusception. This study shows a 11.6% rate of intussusception associated with GJT at our institution, and dramatic increase in risk of repeated intussusception if the GJT remains in place. Our study also highlights that some patients with repeated complications associated with GJT may be able to successfully return to gastric feedings.
Table 1: Clinical Characteristics
Table 2: Tube Status at the Time of Last Follow-Up

.jpg)
.jpg)
