698 - Oxygen Exposure is Associated with Increased Risk of Necrotizing Enterocolitis in Premature Infants
Friday, April 24, 2026
5:30pm - 8:00pm ET
Publication Number: 1675.698
C. Abigail. Temple, Boston Children's Hospital, Boston, MA, United States; Erika M. Edwards, Vermont Oxford Network, Burlington, VT, United States; Danielle Ehret, Robert Larner, M.D., College of Medicine at the University of Vermont, Burlington, VT, United States; Amy E.. O‘Connell, Boston Children's Hospital, Boston, MA, United States
Resident Boston Children's Hospital Boston, Massachusetts, United States
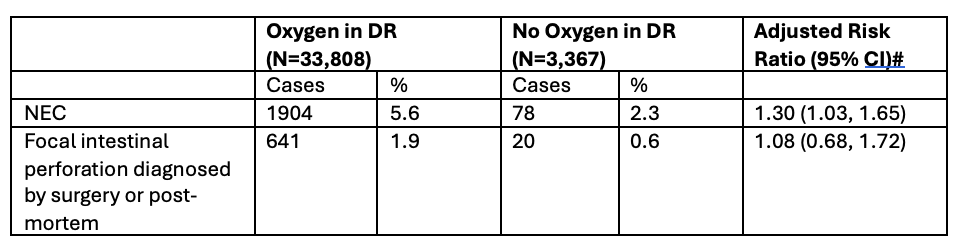
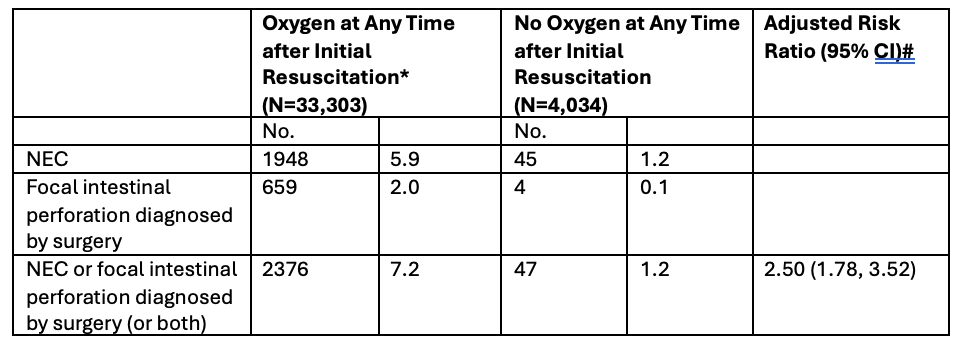
Background: Necrotizing enterocolitis (NEC) is a disease of intestinal inflammation and necrosis affecting ~5-8% of premature infants. While it is a significant contributor to infant mortality and complications both in the NICU and following discharge, its pathogenesis is not fully characterized. NEC does not occur in-utero and typically occurs 7-32 days after birth. This timeline suggests a critical role of postnatal exposures in pathogenesis. While some studies have suggested a role of acute intermittent hypoxia in inciting NEC, others have begun to consider a role for chronic hyperoxia in damage via reactive oxygen species and alterations in intestinal development, which may predispose the intestine to development of NEC. However, clinical correlation has not been directly evaluated in the literature. Objective: To assess if an association exists between postnatal oxygen exposure and risk of developing NEC in premature infants. Incidence of spontaneous focal intestinal perforation (SIP) was also evaluated as a comparator, since these disorders have different pathogenesis. Design/Methods: Infants born < 1501 grams in 2024 with a total length of stay of at least four days and reported to Vermont Oxford Network were included. NEC was diagnosed at surgery, at postmortem examination or by at least one clinical sign (bilious gastric aspirate or emesis; abdominal distension or discoloration; occult or gross blood in stool) and at least one diagnostic imaging finding (pneumatosis intestinalis; hepato-biliary gas; pneumoperitoneum). Surgically confirmed SIP was defined as focal intestinal perforation separate from NEC based on visual inspection of the bowel at surgery or post-mortem. Generalized estimating equation logistic regression were used to estimate risk ratios adjusted for gestational age, small for gestational age, sex, multiple birth, inborn at the reporting hospital, cesarean delivery, 1-minute Apgar score, and clustering of infants within hospitals. Results: There is increased risk of developing NEC in infants exposed to oxygen in the delivery room (ARR 1.30, CI 1.03-1.65), infants exposed at any time after initial resuscitation (ARR 2.50, CI 1.78-3.52), infants exposed after the delivery and before 28 days (ARR 1.76, CI 1.21- 2.57), and infants exposed on day 28 (ARR 1.55, CI 1.35-1.78) compared to non-exposed infants. There is not an increased risk of developing SIP in infants exposed to oxygen at any time.
Conclusion(s): There is an association between oxygen exposure and NEC. Further studies should be conducted to determine if there is an association between total oxygen exposure and NEC risk.
Table 1: Risk of NEC and SIP with Oxygen Exposure in the Delivery Room
Table 2: Risk of NEC with Oxygen Exposure at Any Time Point After Initial Resuscitation
Tables 3a-3b: Risk of NEC with Oxygen Exposure for <28 Days and on Day 28 in the NICU

 photo")