591 - Rethinking Discharge: Rapid Emergency Aftercare by Telehealth (REACT) for Children
Friday, April 24, 2026
5:30pm - 8:00pm ET
Publication Number: 1568.591
Evie K. Cannon, Monroe Carell Jr. Children's Hospital at Vanderbilt, Nashville, TN, United States; Allyson Bost, Monroe Carell Jr. Children's Hospital at Vanderbilt, Lebanon, TN, United States; Jennifer Jones, Monroe Carell Jr. Children's Hospital at Vanderbilt, Nashville, TN, United States; Michele Walsh, Monroe Carell Jr. Children's Hospital at Vanderbilt, FRANKLIN, TN, United States; Barron Frazier, Monroe Carell Jr. Children's Hospital at Vanderbilt, Nashville, TN, United States
Resident Monroe Carell Jr. Children's Hospital at Vanderbilt Nashville, Tennessee, United States
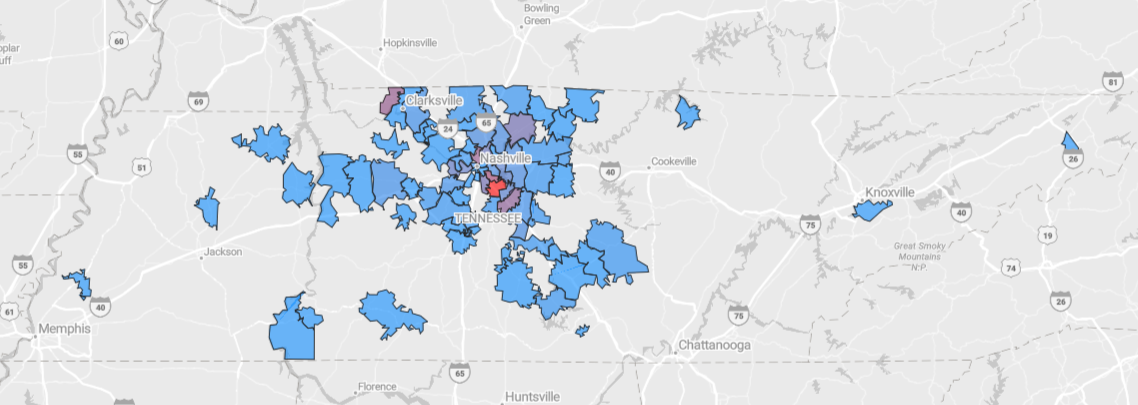
Background: Return visits to pediatric emergency departments (ED) increase strain on families and the healthcare system, contributing to longer wait times, increased costs, and reduced satisfaction. The Rapid Emergency Aftercare by Telehealth (REACT) program is a novel, provider-initiated service offering timely follow-up after ED discharge. REACT visits are conducted by existing ED advanced practice providers during low-volume morning hours. Objective: The REACT program targets patients needing closer monitoring, additional evaluation, or reassurance, aiming to improve continuity of care, supplement healthcare access, and reduce unnecessary return ED visits. Design/Methods: We conducted a retrospective analysis of REACT telehealth follow-up encounters at a single quaternary children's hospital from May 1 to September 30, 2025. Descriptive statistics summarized demographics, visit characteristics, and completion rates by insurance type, language, age, and month. Multivariable logistic regression was used to identify predictors of visit completion, adjusting for age, gender, language, insurance, ethnicity, ED-to-telehealth lag, month, and diagnosis category. Adjusted odds ratios (ORs), 95% confidence intervals (CIs), and p-values were reported. Results: A total of 233 records were analyzed. The mean age was 44 months, with most patients being English-speaking (83%) and covered by Medicaid (63%). Geographic distribution of patients using REACT was visualized using a ZIP code heatmap (Figure 1). REACT visit completion rate was 61%, with 39% canceled or incomplete. Time from ED presentation to REACT visit was a median of 2 days (IQR 1-2) with a mean of 1.89 days. ED-Telehealth lag per day was statistically significant with OR of 0.69, CI: 0.52-0.90 (p=0.007). Visit durations averaged 12.1 minutes with a median of 10 minutes (IQR 10-15, n=142). ED return rate within 72 hours for patients with completed REACT visits was 6.3%. The top visit diagnoses include croup, bronchiolitis, viral gastroenteritis, viral illness, fever, and rash.
Conclusion(s): REACT offers a successful reimagining of post-ED care by providing rapid telehealth follow-up with the benefit of baseline ED insight. Using existing ED staff during low-volume morning hours makes the model scalable and practical. While visit completion rates remain a focus for improvement, REACT shows promise in enhancing continuity of care and satisfaction. Future efforts include REACT visit surveys to guide program refinement and assess experience.

 photo")