55 - In-Hospital Outcomes for Preterm Infants with Neonatal Encephalopathy
Friday, April 24, 2026
5:30pm - 8:00pm ET
Publication Number: 1048.55
Sarah A. Martin, Primary Children's Hospital, Salt Lake City, UT, United States; Tara L. DuPont, University of Utah School of Medicine, Salt Lake City, UT, United States; Con Yee Ling, University of Utah School of Medicine, Salt Lake City, UT, United States
Fellow Primary Children's Hospital Salt Lake City, Utah, United States
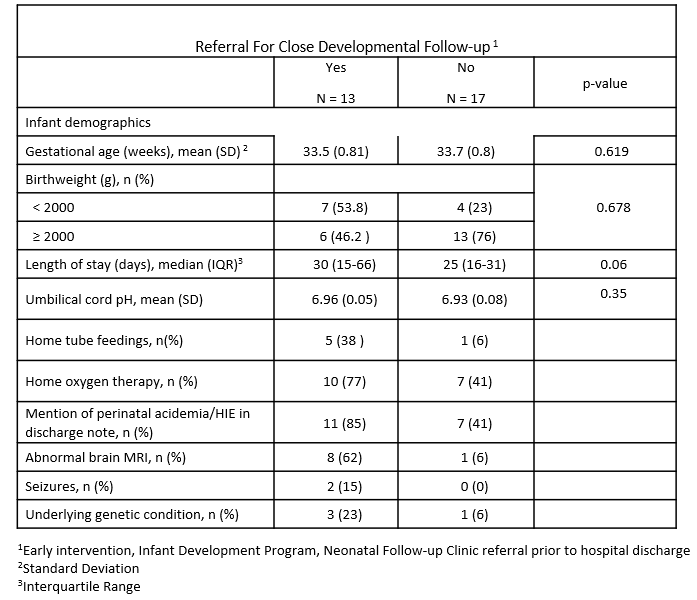
Background: Previous studies have reported an incidence of HIE in about ~6 per 1000 live births for infants born at 32-35 weeks. The Sarnat exam has been validated down to 32 weeks of gestation; however, there are no approved neuroprotective therapies for preterm infants with evidence of HIE. While no therapeutics are available for infants 32-35 weeks with HIE, they may benefit from early intervention services and close monitoring of development. Objective: Evaluate and describe in-hospital outcomes in preterm infants with severe perinatal acidemia born between 32 and 35 weeks. Design/Methods: This retrospective analysis included infants born between 32- and 35-weeks from a previously established hospital system dataset between Jan.1st, 2021 and July 31st, 2025. Infants were included if they had an umbilical cord gas pH ≤ 7.0 or base deficit of >16. Descriptive statistics were performed and analyzed. Continuous data was analyzed with two-tailed Student's T-tests, and categorical risk factors were analyzed with chi-squared or Fisher's exact tests. Results: We identified 30 newborns with an umbilical cord gas pH ≤7.0 or base deficit >16. The average gestational age was 33.6 ±0.81 weeks, the average birthweight was 2199 ± 575 grams and average umbilical cord gas pH was 6.94 ± 0.07. In 25 infants (88.3%), an identifiable perinatal event preceded delivery. Two infants included in this cohort had a documented Sarnat examination and one infant underwent therapeutic hypothermia. There were 12 infants (40%) that experienced an abnormal short-term hospital outcome, including home nasogastric tube feedings (n=4), gastrostomy tube placement prior to hospital discharge (n=2), abnormal brain MRI (n=9), seizures (n=2) failed hearing screen (n=2), or death (n=1). Four infants were found to have an underlying genetic condition. Eighteen (60%) infants had a diagnosis of perinatal acidemia or HIE documented in the hospital discharge note. Nine infants had referrals for developmental follow-up programs (Table 1).
Conclusion(s): In this review of preterm infants born between 32 and 35 weeks with severe perinatal acidemia, almost half of the infants experienced an abnormal short-term hospital outcome; yet only 30% of infants were referred to a developmental follow-up program. This data suggests that preterm infants with severe perinatal acidemia may be receiving less attention to long-term development than their term counterparts. Future efforts could be directed at improving the diagnosis of perinatal acidemia with subsequent referral for developmental follow-up at the time of discharge.
Table 1: Infant Characteristics By Referral for Close Developmental Follow-up