592 - Predictors of Emesis in Children with Ketamine Procedural Sedation: Is Pretreatment with Zofran Indicated?
Friday, April 24, 2026
5:30pm - 8:00pm ET
Publication Number: 1569.592
Sandhia Arrora, Dayton Children's Hospital, Dayton, OH, United States; Ramzi Nahhas, Wright State University Boonshoft School of Medicine, Dayton, OH, United States; Medhavi Anand, Wright State University Boonshoft School of Medicine, Beavercreek, OH, United States; Samantha Gilbert, Dayton Children's Hospital, Beavercreek, OH, United States; Anisha Mandava, Wright State University Boonshoft School of Medicine, Beavercreek, OH, United States; Ashima Goyal Gurkha, Dayton Children's Hospital, Dayton, OH, United States
PEM Fellow Dayton Children's Hospital Dayton, Ohio, United States
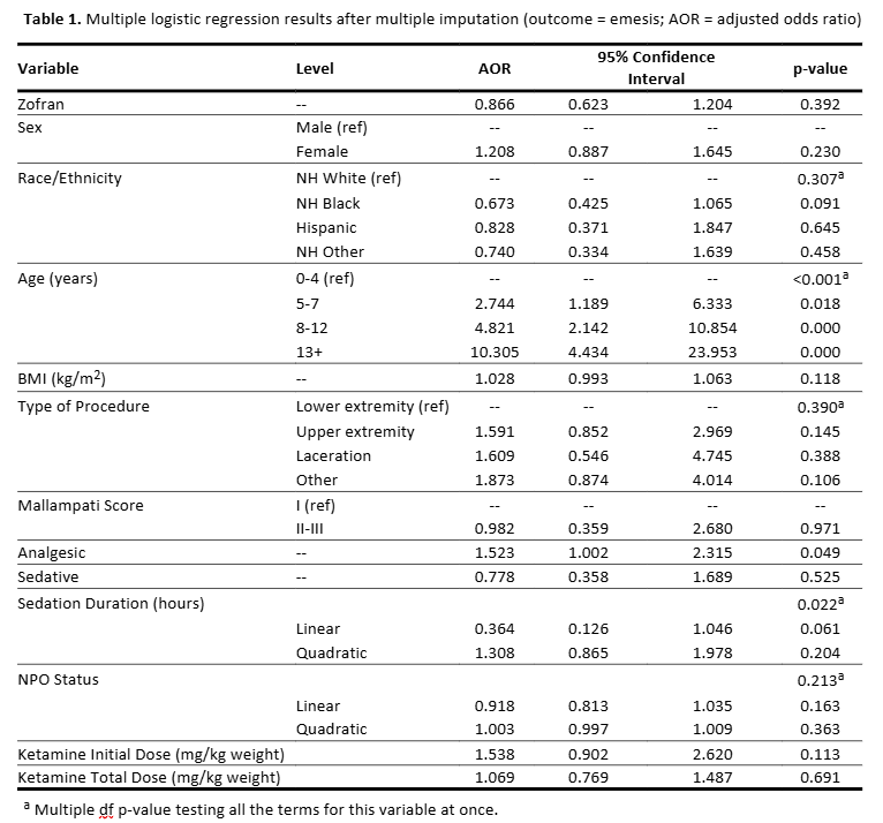
Background: Ketamine is the most commonly used agent for pediatric procedural sedation and analgesia (PSA) in the emergency department. However, despite its generally favorable safety profile, ketamine can cause unintended side effects such as nausea and emesis. Prior studies have identified various predictors of emesis during ketamine procedural sedation. Moreover, despite the widespread use of Zofran, there is limited evidence regarding its effectiveness in preventing emesis during sedation. Objective: This study aimed to evaluate the effect of Zofran pretreatment on the odds of emesis and to characterize patient variables among pediatric patients who received ketamine for procedural sedation. Design/Methods: We conducted a retrospective cohort study from January 1, 2019, to December 31, 2024, using electronic medical records of patients aged 6 months to 21 years who received ketamine for procedural sedation. Patients were excluded if ketamine was administered for multi-system trauma. We defined emesis as: one or more episodes of nausea or vomiting post ketamine administration before emergency department discharge or admission. Descriptive statistics were used to summarize clinical characteristics. Logistic regression and propensity score analysis were used to estimate the association between Zofran and emesis, adjusting for potential confounders. Multiple imputation was used to address missing data. Results: Our study period included 2,946 patients. After excluding 14 patients, the sample size was 2,932, of whom 2,212 (75.4%) received Zofran. Emesis occurred in 163 (7.4%) patients who received Zofran and in 55 (7.7%) who did not. Based on the propensity score analysis, those who were administered Zofran with ketamine had 13.3% lower odds of emesis than those who were not, the difference was not statistically significant (adjusted odds ratio = 0.867, 95% CI = 0.628, 1.196, p = 0.384). Logistic regression analysis results matched the propensity score results. Predictors significantly associated with greater odds of emesis were age >=5 years, co-administration analgesic use, and shorter sedation duration (Table 1).
Conclusion(s): Our study observed a beneficial effect of Zofran in decreasing the odds of emesis with ketamine sedation; however, the effect size was not statistically significant. Future studies should evaluate the use of Zofran in a larger sample to better assess its potential benefit.
Table 1: Multiple logistic regression after multiple imputation

 photo")