53 - Feasibility of Cerebral Cytochrome C Oxidase Monitoring in Newborns Using FlexNIRS
Friday, April 24, 2026
5:30pm - 8:00pm ET
Publication Number: 1046.53
Julia Davis, MassGeneral Hospital for Children, Cambridge, MA, United States; John Sunwoo, Brigham and Women's Hospital / Harvard Medical School, Boston, MA, United States; Nikola Otic, MGH, Boston, MA, United States; Olivia S. Kierul, Massachusetts General Hospital, Boston, MA, United States; Marco Renna, Massachusetts General Hospital, Boston, MA, United States; Maria Angela Franceschini, Massachusetts General Hospital, Harvard Medical School, boston, MA, United States; Emily M. Herzberg, Mass General Brigham for Children / Harvard Medical School, Lynnfield, MA, United States
Clinical Research Coordinator MassGeneral Hospital for Children Cambridge, Massachusetts, United States
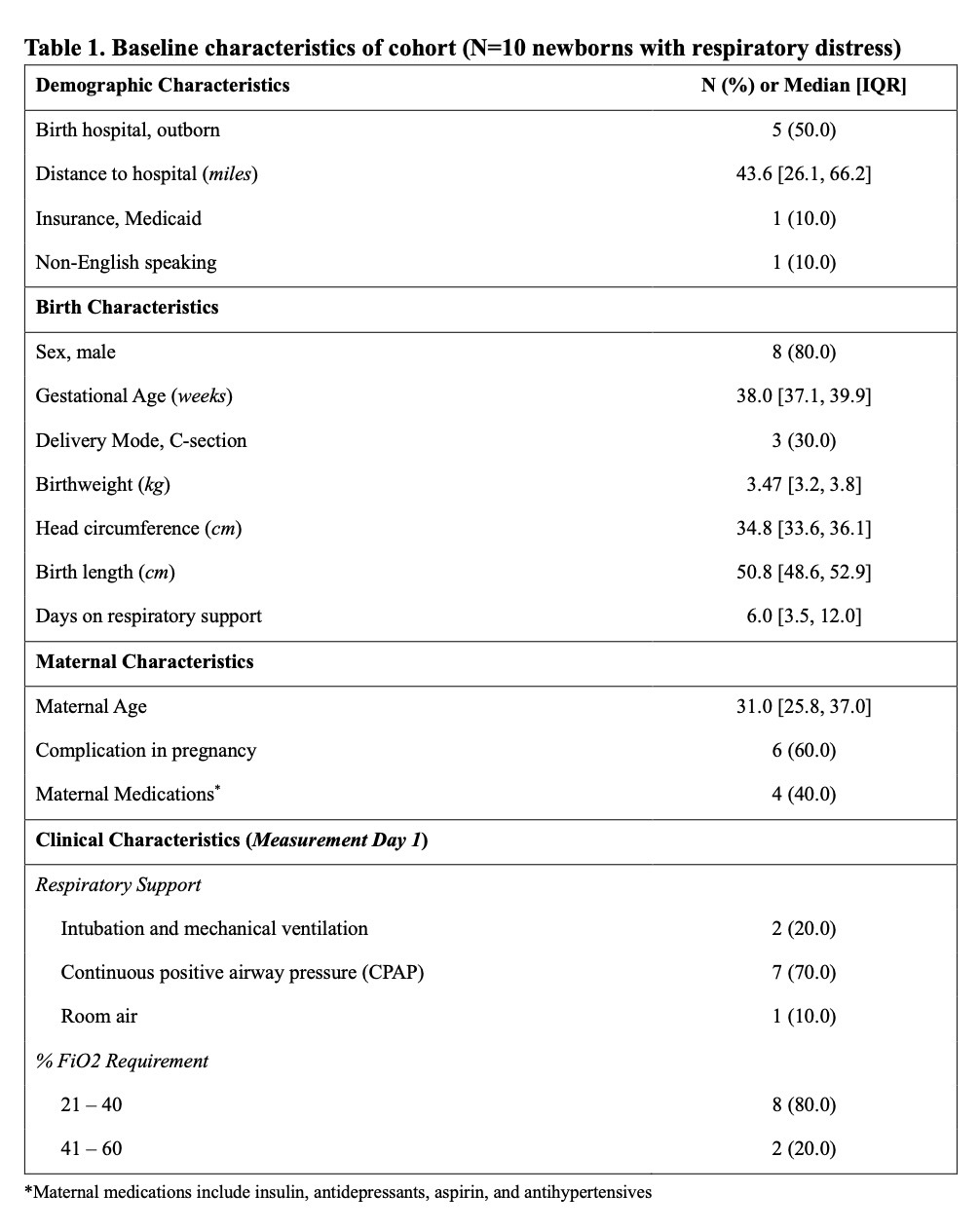
Background: Continuous, non-invasive bedside monitors are essential for guiding clinical decisions in Neonatal Intensive Care Units (NICUs) (Bale et al., 2016). Near-infrared spectroscopy (NIRS) allows for bedside assessment of biological variables, including oxidized cytochrome c oxidase (oxCCO), a marker of cerebral metabolism (Hunter et al., 2018). Previous studies have shown that mitochondrial metabolism remains stable during brief desaturation events in healthy newborn brains (Bale et al., 2019). Objective: 1) Validate a multi-wavelength (MW)-FlexNIRS device for measuring changes in oxCCO in newborns with transient respiratory distress and 2) assess the relationship between ΔoxCCO and periods of oxygen desaturation. Ultimately, we aim to establish feasibility of MW-FlexNIRS-oxCCO monitoring in neonates with hypoxic-ischemic encephalopathy (HIE) and potential brain injury. Design/Methods: We enrolled 10 newborns (≥36 weeks gestation, ≤28 days old) with respiratory distress from the Massachusetts General Hospital NICU. Changes in oxCCO (ΔoxCCO) were measured using MW-FlexNIRS, a battery-operated wireless NIRS wearable device developed by our team (Wu et al., 2022), and co-registered with a pulse oximeter. The MW-FlexNIRS hosts two 8-wavelength LED modules (735 nm-910 nm) and four photodiode detectors, sampling each source-detector pair at 40 Hz. The device conforms to the newborn forehead. Newborns were monitored for up to 12 hours/day for up to 3 days. Light intensity waveforms were cleaned for ambient light/motion artifacts, then converted to cerebral oxygenation (ΔOxy), blood volume/perfusion (ΔHbT), and ΔoxCCO using a diffusion-based (g1) model linking tissue absorption and scattering to measured light intensity. A slow cubic trend was removed from daily concentration estimates. Desaturations were defined as SpO2 < 90%; ΔOxy, ΔHbT, & ΔoxCCO response was compared. Results: The majority (70%) received CPAP with low oxygen requirement during monitoring (Table 1). 9/10 newborns had at least one desaturation event, averaging 3 ± 2 minutes and were included in analysis. We demonstrate a correlation trend between cerebral oxygenation and SpO2, while oxCCO concentration was stable during desaturation events (Figure 1).
Conclusion(s): We found that cerebral metabolism remains stable during brief desaturation events in newborns without brain injury, confirming prior work and demonstrating feasibility of MW-FlexNIRS in the NICU. Future steps will apply MW-FlexNIRS-oxCCO monitoring in newborns with HIE, to enable earlier brain injury detection and faster, individualized intervention.
Table 1. Baseline characteristics of cohort (N=10 newborns with respiratory distress)
Figure 1. Change in cerebral measurements in 9 neonates with 33 desaturation events

 photo")
.jpg)
