Associate Professor Children's Hospital Colorado Denver, Colorado, United States
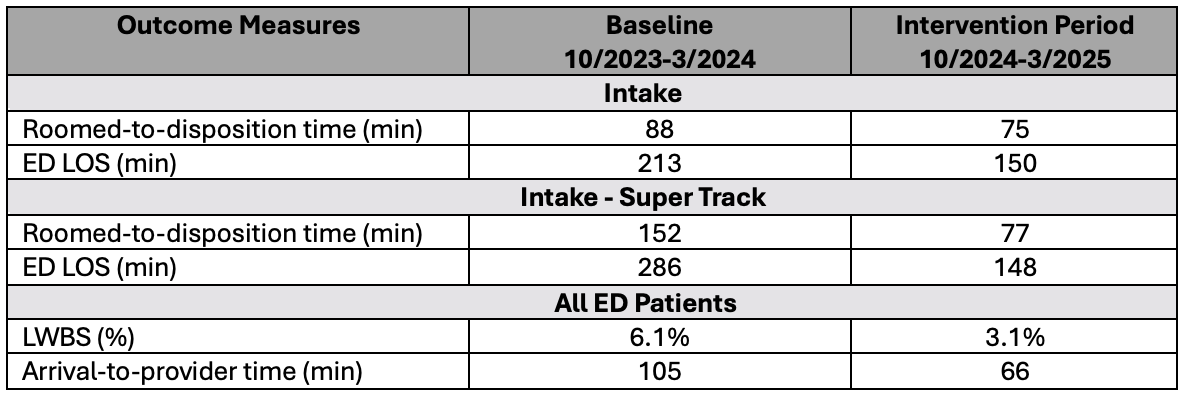
Background: Emergency Department (ED) crowding remains a national challenge, contributing to care delays, longer length of stay (LOS), and higher rates of patients leaving without being seen (LWBS). Front-end strategies such as Intake and split-flow models can improve throughput by enabling earlier assessment and disposition. Building on our prior Intake model, this quality improvement (QI) initiative sought to enhance patient flow by introducing alternate care spaces to allow continued management of Intake patients needing focused, straightforward interventions while preserving main ED capacity for higher-acuity care. Objective: This QI initiative aims to reduce roomed-to-disposition time for patients in Intake by 10% from October 22, 2024 - February 28, 2025. Design/Methods: This QI initiative was conducted in a pediatric ED at a quaternary care, level I trauma center with a physician-driven Intake model. The primary intervention was the addition of new care chairs adjacent to Intake, serving as a dedicated space for advancing care of patients requiring focused interventions while remaining under the Intake physician. For situational awareness, these patients were labeled "Super Track" in the electronic health record. The chairs were used for results waiting and continued treatment. Additional interventions included role clarification, standardized workflows, and targeted staff education. The primary outcome was roomed-to-disposition decision time for all Intake patients, with a goal reduction of 10%. Secondary outcomes included LOS, arrival-to-provider time, and LWBS rate. The primary process measure was average time in first room, with a balancing measure of percentage of patients returning within 72 hours. Individual charts (I-charts) were used to continuously monitor outcomes. Results: During the intervention period, 5,618 patients were seen in Intake. Roomed-to-disposition time for all Intake patients decreased by 15% (88 to 75 min), while the focused-intervention patients experienced a 49% reduction (152 to 77 min). LOS for all Intake patients decreased by 30% (213 to 150 min), and by 48% for the focused-intervention patients (286 to 148 min). Additional improvements included a 49% reduction in LWBS rates and a 37% decrease in arrival-to-provider time across all ED patients. 72-hour return visits remained stable during intervention.
Conclusion(s): Our QI initiative demonstrated that strategic reorganization of existing ED front-end processes, without the need for additional staffing or physical expansion, can lead to meaningful improvements in patient throughput, provider efficiency, and overall ED performance.
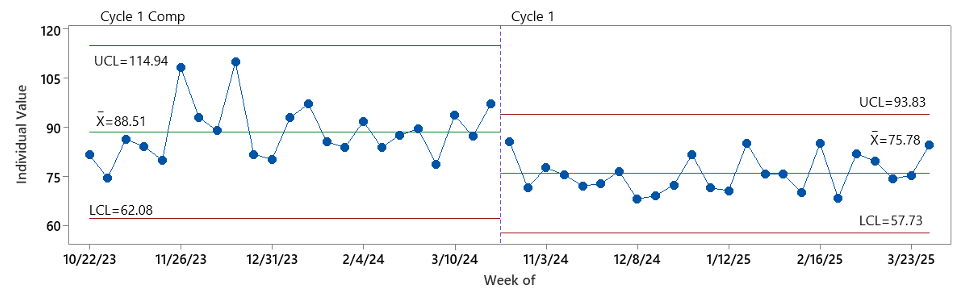
Figure 1: Average Roomed-to-Disposition Time - All Intake Patients
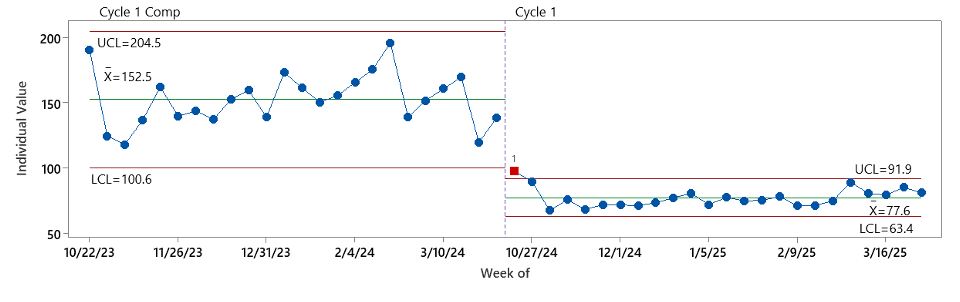
Figure 2: Average Roomed-to-Disposition Time - Intake - Super Track Patients
Table: Outcome Measures During Baseline and Intervention Periods

 photo")