Children's Hospital of Fudan University Shanghai, Shanghai, China (People's Republic)
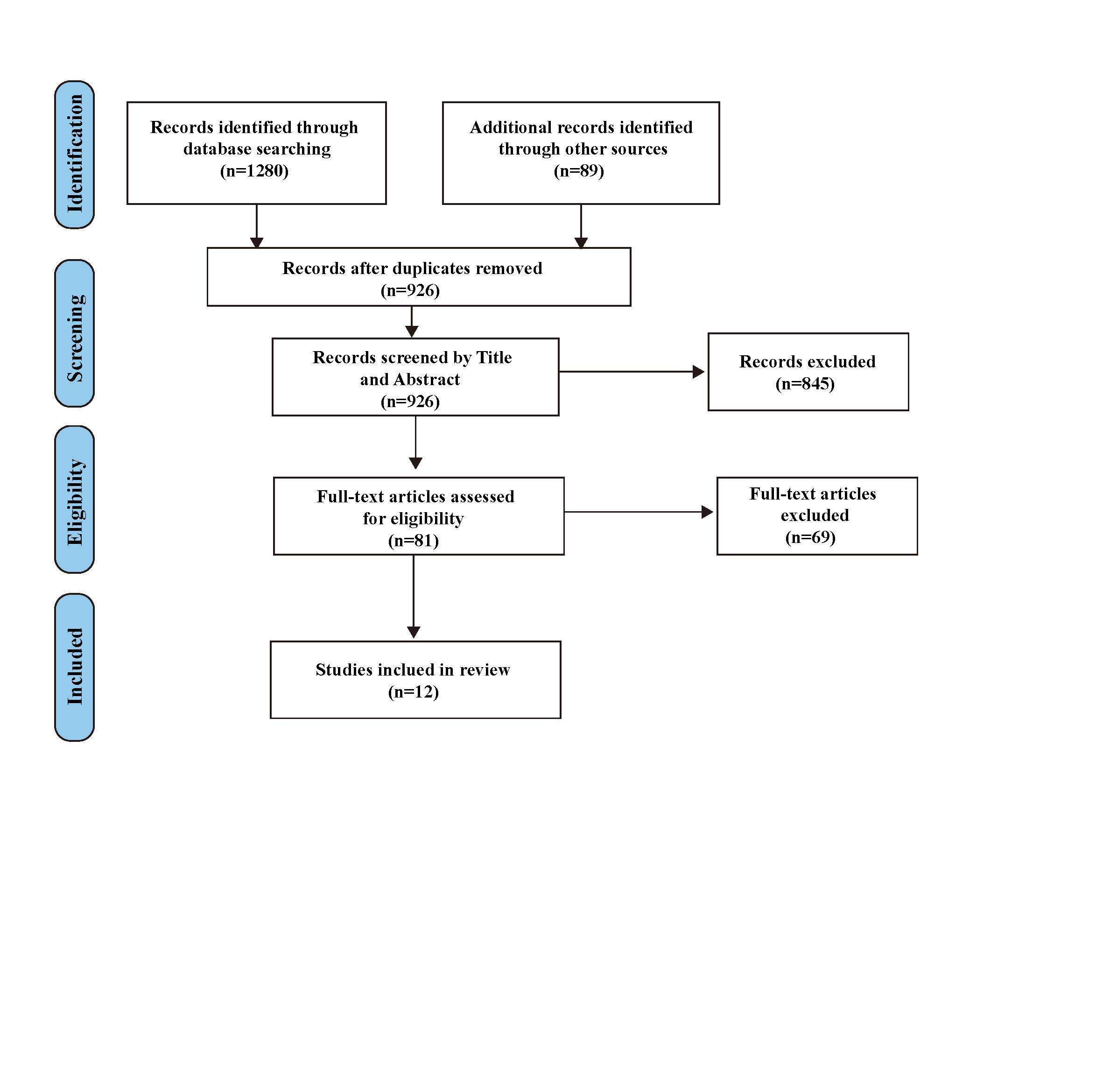
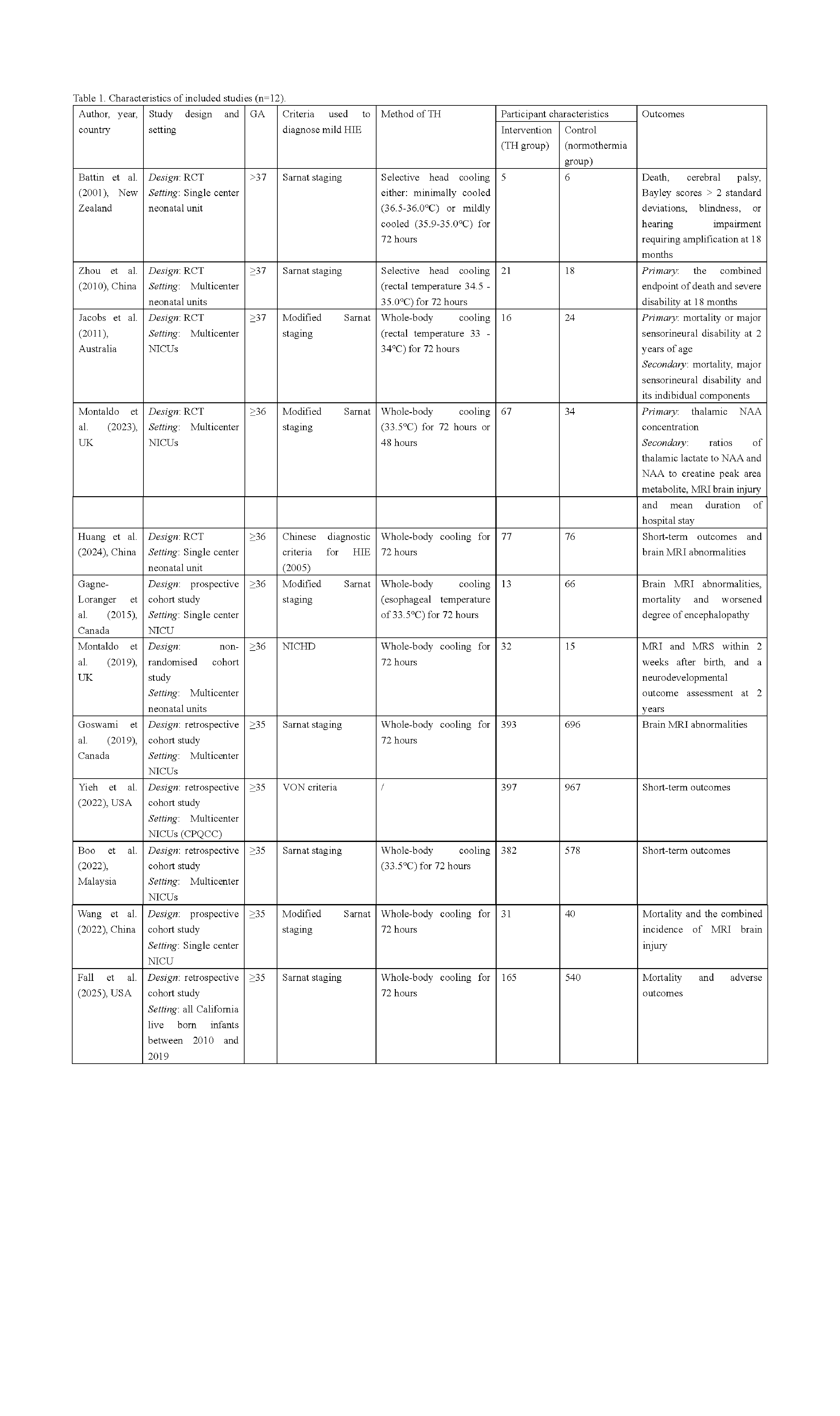
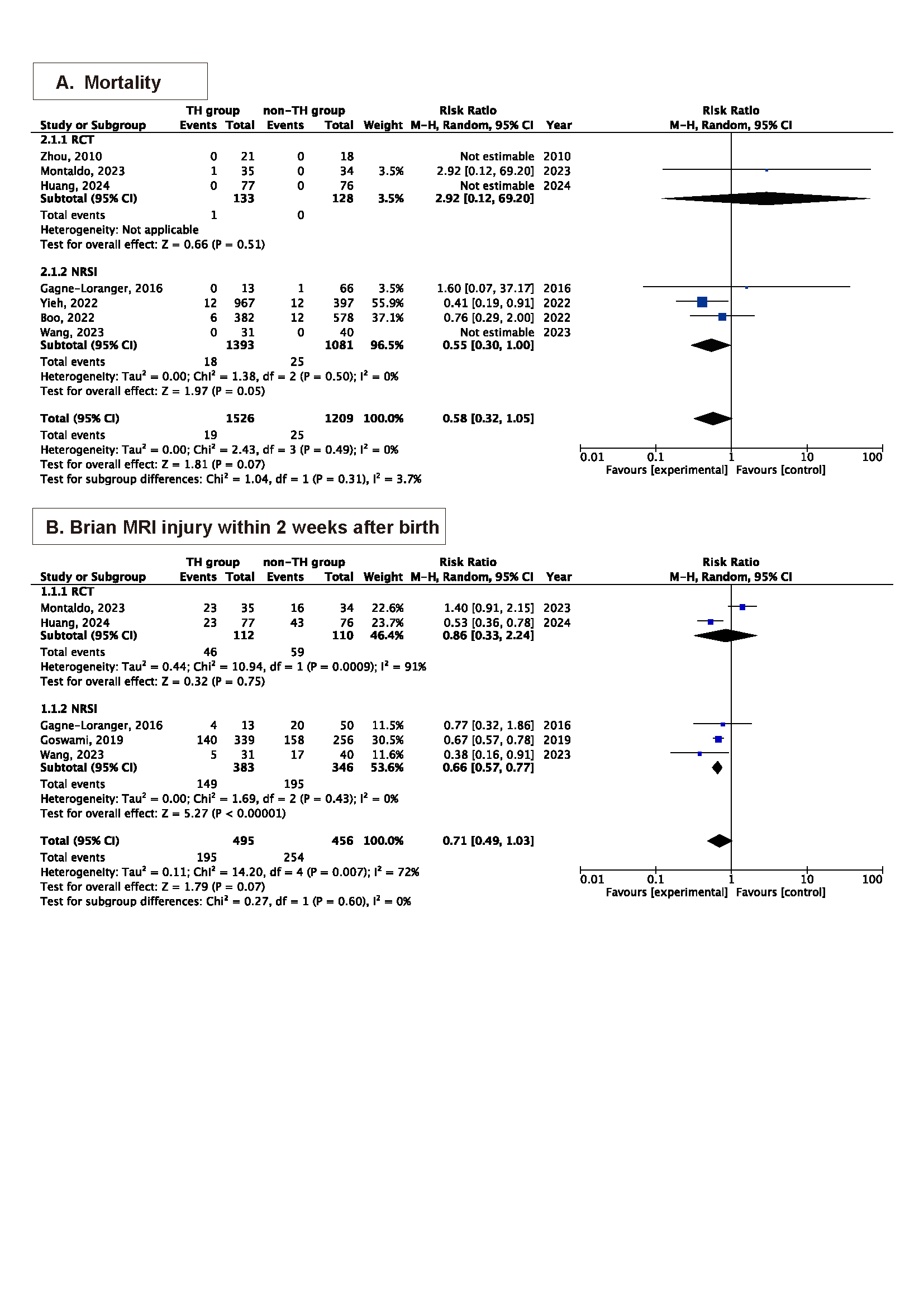
Background: The use of therapeutic hypothermia (TH) in babies with mild hypoxic-ischemic encephalopathy (HIE) is creeping into clinical practice despite a lack of evidence. Previous meta-analyses have predominantly included randomized controlled trials (RCTs) focusing on patients with moderate to severe HIE, resulting in limited sample sizes and few analyzable outcomes specifically relevant to mild HIE. Furthermore, the first RCT dedicated to mild HIE emerged in 2023. To date, no systematic review has comprehensively synthesized the findings from these recent studies. Objective: This study aimed to evaluate the efficacy and safety of TH in neonates with mild HIE. Design/Methods: We conducted a systematic review and meta-analysis. We searched electronic databases and trial registries (MEDLINE, CINAHL, Embase, Web of Science, and CENTRAL) until October 15, 2025, for studies comparing TH and non-feeding strategies. We performed a random-effects meta-analysis using Rev-Man 5.4 software. The primary outcome was mortality and brain MRI injury within 2 weeks after birth. Other outcomes included MRI injury of various brain regions, MRS abnormity, seizures, long-term severe disability, worsen encephalopathy degree and other adverse outcomes. Certainty of evidence was assessed with Grading of Recommendations Assessment, Development, and Evaluation. This study is registered with PROSPERO, CRD420251179187. Results: Twelve studies (five randomized controlled trials (RCTs) and seven nonrandomized studies of intervention (NRSIs)) enrolling 4,659 participants were included. No clear evidence was found of difference in mortality in RCTs (risk ratio [RR] 2.91 [95% CI 0.12 -69.20]) and NRSIs (0.55 [0.30 to 1.00]). In the NRSIs, TH reduced the risk of brain injury on MRI within 2 weeks after birth (0.66 [0.57-0.77]), especially white matter injury (0.53 [0.39-0.72]). No statistically significant differences were observed in long-term neurodevelopmental outcomes, though the evidence was of low or very low certainty. Infants in TH group had higher risk of several short-term complications, including need for respiratory support, arrhythmia, opioid use, abnormal clotting, persistent pulmonary hypertension and prolonged hospital stay.
Conclusion(s): This study provides high-certainty evidence that TH reduces brain injury in infants with mild HIE, while also increasing specific short-term risks. These findings support consideration of TH for mild HIE, balanced against its potential harms, and highlight the need for further research focused on long-term functional outcomes.
Fig.1 PRISMA flow diagram
Table 1. Characteristics of included studies (n=12).
Fig.2 Forest plot showing a comparison of (a) all-cause mortality; (b) brain MRI injury within 2 weeks after birth