27 - Outcomes of Infants with Mild Neonatal Encephalopathy treated with Therapeutic Hypothermia: A Single-Center Experience
Friday, April 24, 2026
5:30pm - 8:00pm ET
Publication Number: 1024.27
Yoon-Joo Kim, Brigham and Women’s Hospital, BOSTON CLG, MA, United States; Hoda El-Shibiny, Brigham's Women Hospital, Boston, MA, United States; Mohamed El-Dib, Brigham and Women's Hospital / Harvard Medical School, Boston, MA, United States; Carmina Erdei, Brigham and Women's Hospital and Harvard Medical School, Boston, MA, United States
Research Fellow Brigham and Women’s Hospital BOSTON CLG, Massachusetts, United States
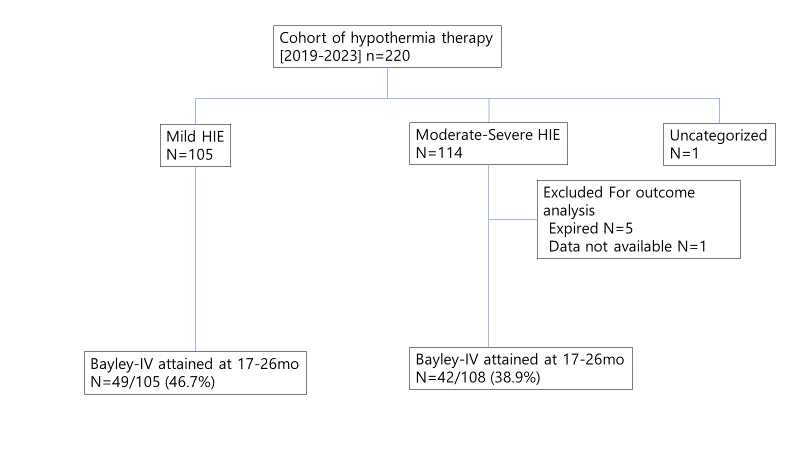
Background: In the post-cooling era, the role of therapeutic hypothermia (TH) in mild neonatal encephalopathy (NE) remains uncertain, with ongoing debate regarding standardized definitions and treatment criteria, and the use of TH in this population. Several studies have reported concerns about brain injury and possibly adverse neurodevelopmental outcomes in infants with mild NE. Objective: To compare neurodevelopmental outcomes of infants with mild versus moderate/severe NE treated with TH in a single academic center over a five years. Design/Methods: This retrospective cohort included infants treated with TH between 2019-2023 based on institutional criteria. Encephalopathy severity was graded using the Neonatal Encephalopathy Scale (NES); a total score ≥ 4 defined eligibility for cooling. Outcomes at two years were compared between mild and moderate/severe NE groups, including the Test of Infant Motor Performance (TIMP) at discharge or at 4 months, Bayley-4 Scales, and Modified Checklist for Autism in Toddlers (M-CHAT) results between 17-26 months. Results: A total of 220 infants received TH during the period, including 105 with mild NE and 114 with moderate/severe NE (Figure 1). Baseline characteristics were notable for a higher rate of placental abruption, lower Apgar scores, lower postnatal ( < 1 h) blood pH, and higher worst NES scores before hypothermia in the moderate/severe group, with other parameters being similar between groups (Table 1). No differences were observed in TIMP scores at hospital discharge or at 4 months. M-CHAT results were comparable (Low risk scores 90.9% vs 82.9%, p=0.46). Bayley-4 showed lower Cognitive and Language standard scores and a trend toward lower Motor scores in the moderate/severe NE group. Among infants with mild NE, up to 21% scored more than 1 SD below the mean across composite domains, and up to 37% scored more than 1 SD below the mean on language or motor subtests (Table 2).
Conclusion(s): Infants with mild NE treated with TH demonstrated overall better neurodevelopment outcomes at two years compared with those with moderate/severe NE. However, a notable proportion of infants with mild NE still scored below the normal range across developmental domains. Although treatment efficacy cannot be inferred based on available data, these findings raise concern for possible developmental vulnerability in this population. The results highlight that more investigation is needed in larger samples of infants with mild NE, to refine eligibility criteria for TH, along with close developmental follow-up post-discharge to better understand and optimize their long-term outcomes.
Figure 1. Flowchart of the study participants
Table 1. Patient characteristics
Table 2. TIMP and Bayley-4 results for neurodevelopmental outcome analysis

 photo")
.png)
.png)
