Session: Neo-Perinatal Health Care Delivery: Practices and Procedures 1
717 - Contrast-Enhanced Head Ultrasound (ceHUS) of the Brain in Neonates: Clinical Utility and Impact on Management
Friday, April 24, 2026
5:30pm - 8:00pm ET
Publication Number: 1694.717
Christhian a. Cano-Guerra, Boston Children's Hospital, Boston, MA, United States; Pallavi Sagar, MassGeneral Hospital for Children, Boston, MA, United States; Teresa Victoria, Mass General Brigham, Boston, MA, United States; Rodica M. Turcu, Harvard Medical School, Boston, MA, United States
Clinical Fellow Boston Children's Hospital Boston, Massachusetts, United States
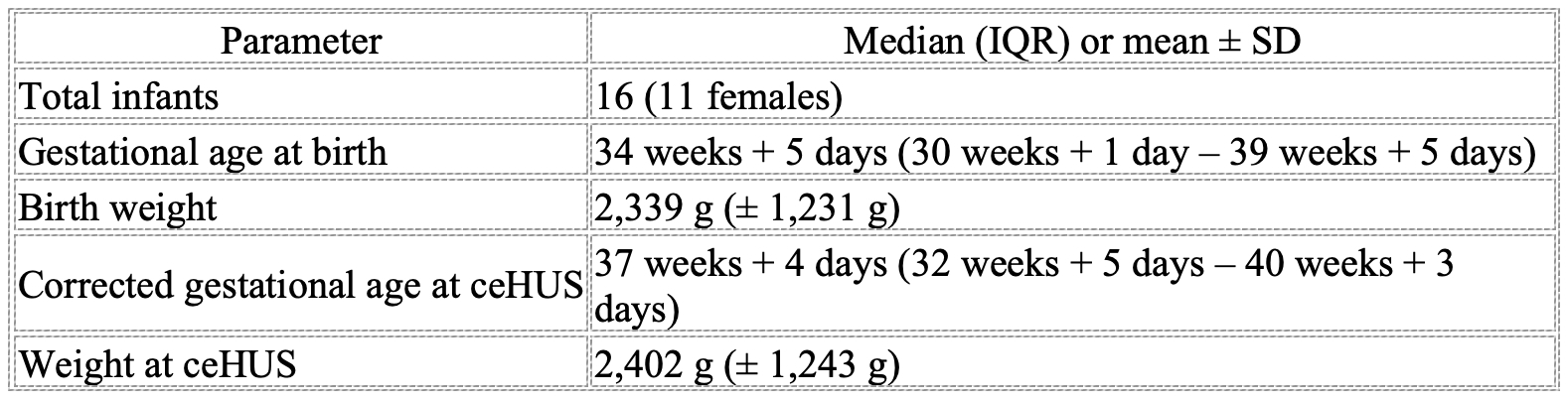
Background: Conventional head ultrasound (HUS) continues to be the first-line neuroimaging modality for diagnosis and management of significant morbidities in the newborn population. Although incredibly useful, conventional HUS has limited sensitivity. Contrast-enhanced ultrasound (ceHUS) overcomes some of the limitations of conventional imaging by using microbubble-based contrast agents with an excellent safety profile. Although it is a promising modality that provides particularly useful information, its use remains limited due to the lack of research and expertise among radiologists and the lack of training among sonographers. Objective: To evaluate the clinical utility of contrast-enhanced head ultrasound (ceHUS) as an adjunct imaging tool for neonatal brain assessment when conventional ultrasound is inconclusive or magnetic resonance imaging (MRI) cannot be obtained. Design/Methods: A retrospective, single-center review was conducted of infants admitted to a level IV neonatal intensive care unit between January 2024 and October 2025 who underwent conventional head ultrasound (HUS) followed by ceHUS using sulfur hexafluoride lipid-type A microspheres (Lumason®). Demographic data, clinical indications, imaging findings, and management decisions before and after ceHUS were analyzed to assess its diagnostic and therapeutic impact. Results: Sixteen infants (11 female) met inclusion criteria. Median gestational age at birth was 34 weeks + 5 days (IQR 30 + 1-39 + 5) and mean birth weight 2,339 g. At the time of ceHUS, corrected median gestational age was 37 weeks + 4 days (IQR 32 + 5-40 + 3) and mean weight 2,402 g. ceHUS indications were grouped as follows: (1) Suspected CNS infection (n = 6); infection-related enhancement was excluded in all cases, leading to antibiotic adjustment; MRI was avoided in five and confirmed findings in one. (2) Hemorrhagic or ischemic lesions (n = 10); ceHUS improved lesion characterization and vascular assessment, detecting arterial or venous occlusions and avoiding unnecessary imaging in one case. MRI was concordant in all but one infant. (3) Perfusion and hemodynamic assessment (n = 3); ceHUS clarified evolving perfusion patterns in cases of cerebral edema, aiding management decisions.
Conclusion(s): ceHUS is a valuable bedside neuroimaging technique providing real-time evaluation of cerebral perfusion and hemodynamics. It enables repeated assessments without patient transport, minimizing physiologic instability and bridging the diagnostic gap between conventional ultrasound and MRI. ceHUS enhances diagnostic confidence and informs management in critically ill neonates.

 photo")