535 - Safety of Peripherally Administered Hypertonic Saline within the Pediatric ICU
Friday, April 24, 2026
5:30pm - 8:00pm ET
Publication Number: 1514.535
Ryan Killebrew, McGovern Medical School at the University of Texas Health Science Center at Houston, HOUSTON, TX, United States; Bibek Bista, McGovern Medical School at the University of Texas Health Science Center at Houston, Houston, TX, United States; Jennifer Nguyen, McGovern Medical School at the University of Texas Health Science Center at Houston, Houston, TX, United States; Vinai Modem, TCU Burnett School of Medicine, Fort Worth, TX, United States; Konstantinos Boukas, McGovern Medical School at the University of Texas Health Science Center at Houston, Houston, TX, United States
Fellow McGovern Medical School at the University of Texas Health Science Center at Houston HOUSTON, Texas, United States
Background: 3% hypertonic saline is commonly used in pediatric patients for increased intracranial pressure and symptomatic hyponatremia. Within the adult population, multiple studies have shown that hypertonic saline can be administered safely via a peripheral line; however, there is a lack of studies in the pediatric population to support this practice. This leads to the establishment of central venous access for administering hypertonic saline, thereby exposing patients to the risks associated with central access. Objective: This study evaluated the safety of peripheral versus central administration of 3% hypertonic saline at a tertiary pediatric hospital, with the hypothesis that hypertonic saline may be safely given via a peripheral IV. Design/Methods: We conducted a retrospective observational study of pediatric ICU patients who received 3% hypertonic saline between January 2021 and December 2025 at Children's Memorial Hermann Hospital. Demographic and clinical data were collected, including vascular access type, indication, method of administration, dose, and documented local complications within one hour of administration. Descriptive statistics summarized patient demographics. Categorical variables were compared using Fisher's exact test, and continuous variables with the Mann-Whitney U test. Logistic regression was performed in the peripheral IV subset to assess associations between method of administration and complication occurrence. Results: A total of 149 unique patients accounted for 190 administrations of 3% hypertonic saline. Peripheral IV access was used in 81 administrations (43%), and central line access in 109 (57%). Local complications occurred in 9 of 81 peripheral administrations (11.1%). All complications were minor, including infiltration (n=5) and phlebitis (n=4). None of the complications required medical or surgical intervention. Univariate logistic regression within the peripheral access subset demonstrated higher odds of complications when both bolus and continuous infusions were administered (OR 18.9, p = 0.008) when compared with the hypertonic saline bolus group.
Conclusion(s): Peripheral administration of 3% hypertonic saline was associated with a low rate of mild, localized complications and no severe events. Complications are more common when intermittent boluses are given while the patient is receiving a continuous infusion through the same peripheral IV line. When appropriately monitored, peripheral administration may represent a safe and practical alternative that reduces the need for central line placement.

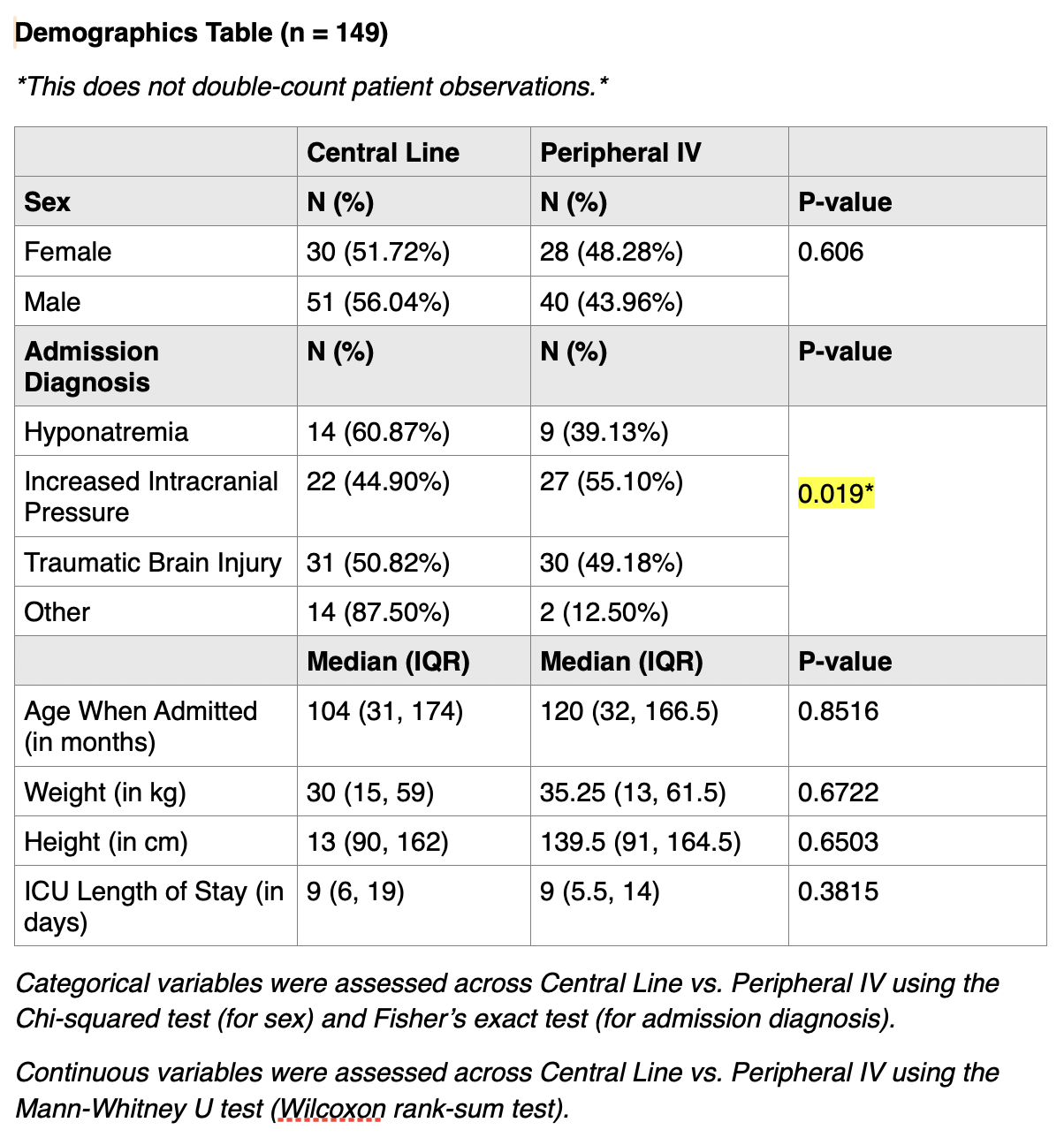 Demographics
Demographics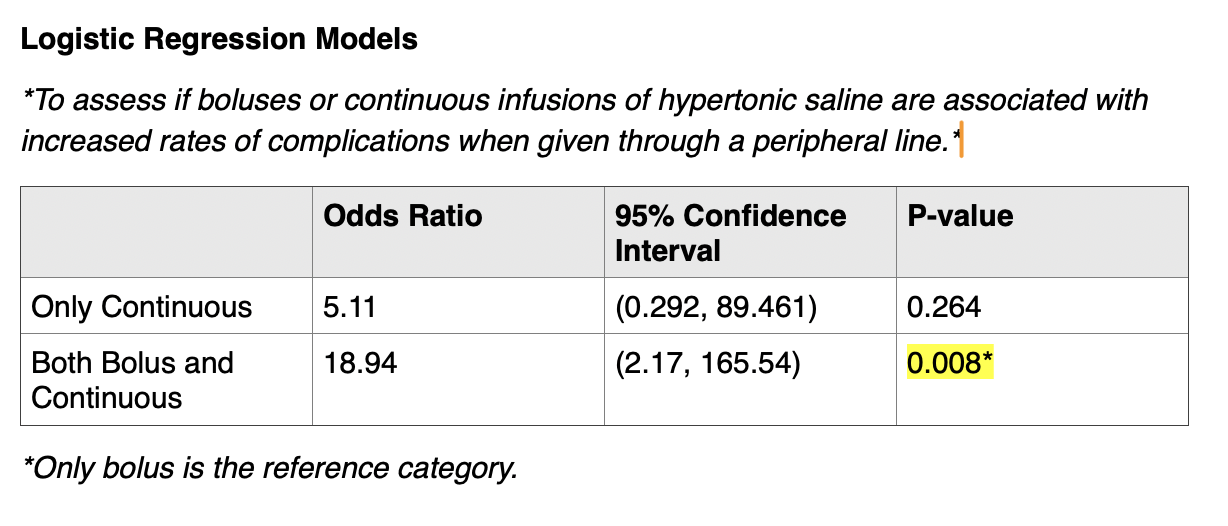 Peripheral IV subset analysis
Peripheral IV subset analysis 