Session: Neo-Perinatal Health Care Delivery: Practices and Procedures 1
720 - Neonatal Urgent Transport-Based Imaging Program (UTIP): Delivering Advanced Imaging Without Children’s Hospital NICU Transfer
Friday, April 24, 2026
5:30pm - 8:00pm ET
Publication Number: 1697.720
Nicholas R. Carr, Intermountain Health, Sandy, UT, United States; Erin Smith, Intermountain Health, Springville, UT, United States; Julie Martinez, Intermountain Health, Murray, UT, United States; Con Yee Ling, University of Utah School of Medicine, Salt Lake City, UT, United States; Erin K. Zinkhan, University of Utah School of Medicine, Salt Lake City, UT, United States; Stevie M. Rowe, Intermountain Health, Provo, UT, United States; Anastasiya Mankouski, Intermountain Health, Salt Lake City, UT, United States; Lori McBride, Intermountain Health Flight and Ambulance Services, Murray, UT, United States; Rosemary A. Valencia, Intermountain Health, Draper, UT, United States; Stacy Reed, Intermountain Health, Murray, UT, United States; Shaun Odell, Intermountain Health, Provo, UT, United States; Stephen D. Minton, Intermountain Health, Provo, UT, United States
Neonatologist, Associate Professor Intermountain Health / University of Utah Sandy, Utah, United States
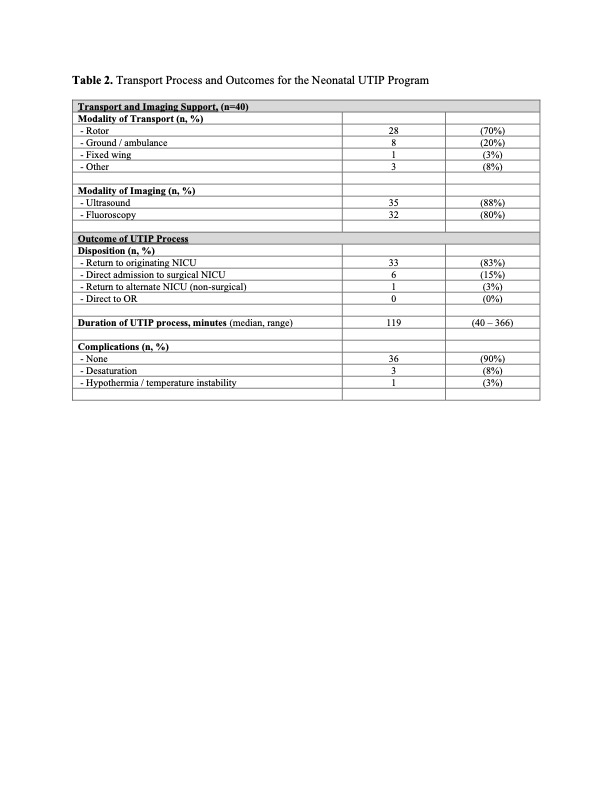
Background: Advanced imaging for critically ill or unstable neonates at community hospitals often requires transfer to surgical or Children's Hospital NICUs, leading to unnecessary bed utilization, care disruption, and family separation. To address these inefficiencies, Intermountain Health established the Neonatal Urgent Transport-Based Imaging Program (UTIP)-a collaborative model integrating neonatal transport, radiology, and telehealth to deliver time-sensitive imaging while maintaining infants in their local facilities whenever feasible. Through real-time telehealth consultation, neonatologists assess infants' clinical stability, including those initially in well newborn nurseries, prior to UTIP activation or NICU admission. Objective: To evaluate implementation, safety, and early outcomes of the UTIP program across a regional neonatal network. Design/Methods: We performed a retrospective review of all UTIP encounters from April 2023-October 2025. Infants were triaged via telehealth assessment or local NICU admission prior to imaging transport. Demographics, indications, transport details, imaging modality, findings, and disposition were collected. Primary outcomes included avoidance of Children's Hospital NICU admission and imaging impact on management. Secondary outcomes included process duration, transport resources, and adverse events. Results: Forty neonates (median gestational age 38.3 weeks [26.6-41.3]; weight 2.85 kg [0.77-4.21]) underwent UTIP imaging. Forty-five percent were preterm, and 52% required respiratory support. Common indications included suspected malrotation or bilious emesis (88%) and intestinal obstruction (23%). Imaging was performed using ultrasound (88%) or fluoroscopy (80%) following rotor (70%) or ground (20%) transport. Median total process time was 119 minutes (range 40-366). No major adverse events occurred; minor events included brief desaturation (8%) and mild temperature instability (3%). Imaging altered management in 13% of cases. Eighty-three percent of infants returned to their referring NICU without Children's Hospital admission; two were directly admitted due to instability, and one remained at parental request.
Conclusion(s): The UTIP program safely delivers advanced imaging to neonates through an integrated transport and telehealth-based model, reducing transfers to surgical centers and preserving family-centered care. This high-value approach enhances access, optimizes system resources, and demonstrates how telehealth-enabled neonatal transport can expand diagnostic capability across regionalized care systems.
Table 1. Patient Characteristics for the Neonatal UTIP Program
Table 2. Transport Process and Outcomes for the Neonatal UTIP Program

.jpg)