596 - Can Pediatric Hospitals Utilize Biometric Technologies to Reunify Separated Families Following a Disaster?
Friday, April 24, 2026
5:30pm - 8:00pm ET
Publication Number: 1573.596
Nathan Reed, Ann & Robert H. Lurie Children's Hospital of Chicago, Evanston, IL, United States; Sara Huston, Ann & Robert H. Lurie Children's Hospital of Chicago, Durham, NC, United States; Diana Madden, Ann & Robert H. Lurie Children's Hospital of Chicago, Evanston, IL, United States; Erica Popovsky, Ann & Robert H. Lurie Children's Hospital of Chicago, Chicago, IL, United States
Student Research Assistant Ann & Robert H. Lurie Children's Hospital of Chicago Evanston, Illinois, United States
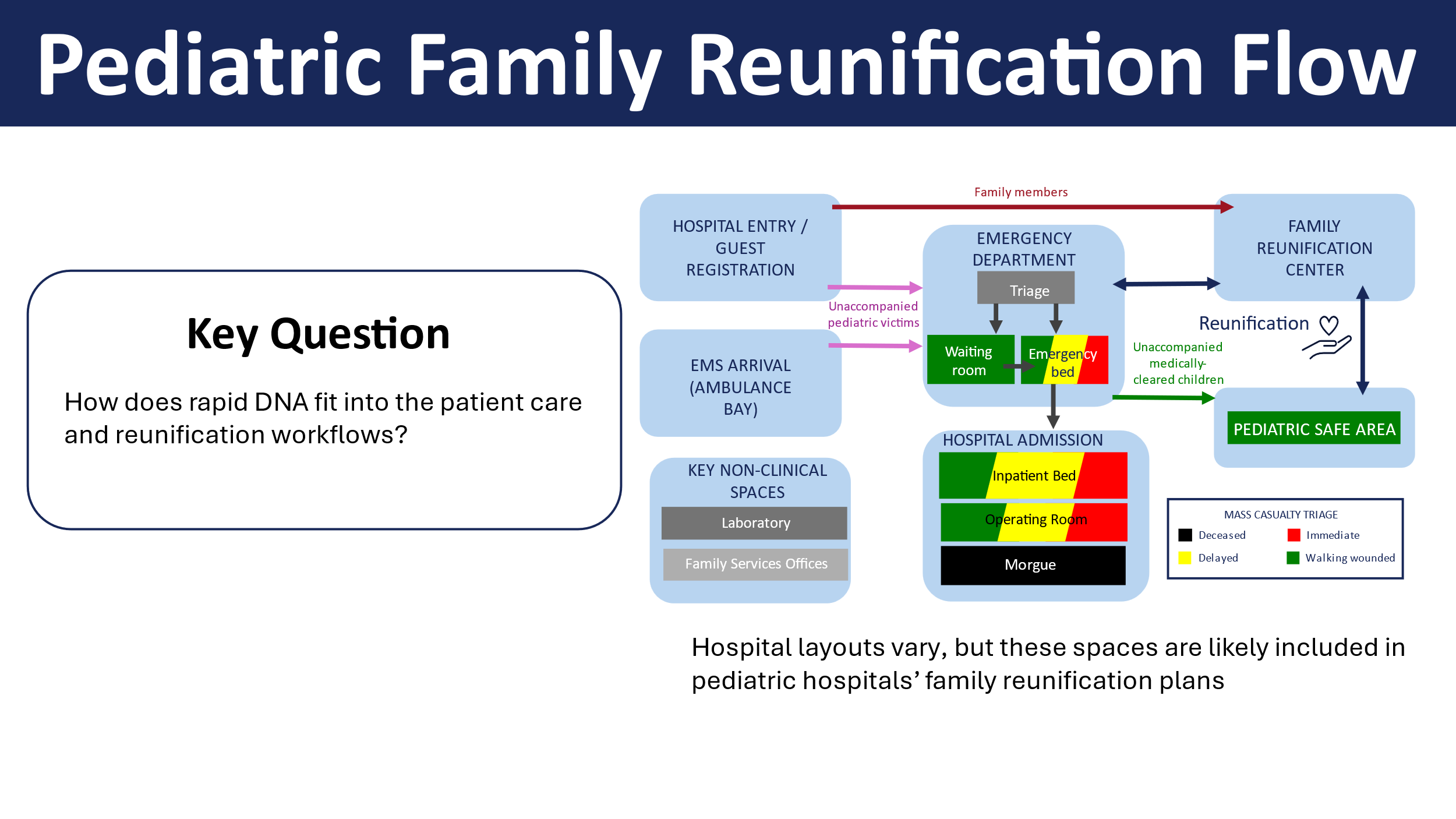
Background: Following a disaster, each hour a child is separated from their caregivers risks their well-being. Biometric tools such as rapid DNA and facial recognition technology (FRT) could greatly enhance the post-disaster pediatric reunification process. Rapid DNA is routinely deployed for postmortem identifications but not currently used in hospitals on living children. A prior survey of 364 caregivers and 131 healthcare providers found support for DNA and FRT for family reunification. Objective: We sought to 1) identify disaster scenarios and timeframes where biometrics could best aid family reunifications and 2) characterize the capabilities and limitations of biometric tools following a disaster. Design/Methods: We developed a set of example scenarios to illustrate the potential use of biometrics, reviewing news sources and government reports to compile details such as timing and scale of the disaster. We noted the capabilities of existing DNA and FRT tools to understand their potential for aiding reunifications. To characterize potential rapid DNA workflow in a hospital, a tabletop reunification exercise was conducted at a stand-alone pediatric hospital. Staff participants completed pre- and post-exercise surveys and recordings of the exercise were analyzed qualitatively. Results: We developed 12 scenarios that illustrate the potential utility of DNA and FRT (Table 1) and generated a decision map (Figure 1). Both FRT and rapid DNA could aid reunification in large-scale disasters with families separated for >24 hours. FRT is best suited for events necessitating multi-site triage. Traditional efforts are likely sufficient for smaller-scale events, with time-limited reunification needs. FRT is not sufficiently validated for children nor on injured faces in a post-disaster context, so it is not ready for deployment. Rapid DNA instruments are limited by capacity (5 samples/90-minute). The tabletop exercise produced a patient flow map (Figure 2) to aid sample workflow. Pre-drill survey of reunification hospital staff (n=22) showed concerns related to chain of custody (41%), sample coordination (41%) and communication of results (32%). Post-survey responses are pending. Open responses show a need to define roles more clearly.
Conclusion(s): Rapid DNA and FRT are not currently utilized in pediatric reunification plans. Rapid DNA might be beneficial in specific scenarios, but the hospital workflow needs to be evaluated. We plan 2 more reunification simulations to evaluate operational workflow. Future research will identify logistics of sampling and testing, sample chain of custody, and personnel allocation and education.
Table 1. Scenarios analyzed to assess utility of biometric tools for pediatric family reunification
Figure 1. Decision map for the use of rapid DNA or FRT following a disaster event Slide1.jpeg
Figure 2. Workflow of family reunification within which Rapid DNA may be employed

 photo")
.png)