521 - Factors associated with recurrent bacterial tracheostomy-associated infection hospitalizations: A multicenter, prospective cohort study
Friday, April 24, 2026
5:30pm - 8:00pm ET
Publication Number: 1501.521
John M. Morrison, Johns Hopkins All Children's Hospital, Saint Petersburg, FL, United States; Naoko Kono, Keck School of Medicine of the University of Southern California, los angeles, CA, United States; Margaret Rush, Children's National Health System, Washington, DC, United States; Andrea Hahn, Children's National Hospital, Washington, DC, United States; Catherine S.. Forster, University of Pittsburgh School of Medicine, Pittsburgh, PA, United States; Jonathan Cogen, University of Washington School of Medicine, Seattle, WA, United States; Joanna Thomson, Cincinnati Children's, Cincinnati, OH, United States; Sarah Hofman DeYoung, University of Washington School of Medicine/Seattle Children's Hospital, Seattle, WA, United States; Krystal Jin, Lucile Packard Children's Hospital Stanford, Palo Alto, CA, United States; Lindsey Scheller, University of California, San Francisco, National Clinician Scholars Program, San Francisco, CA, United States; Rebecca Steuart, Medical College of Wisconsin, Milwaukee, WI, United States; Wendy Mack, University of Southern California, Los Angeles, CA, United States; Michael Neely, Children's Hospital Los Angeles, Los Angeles, CA, United States; Tamara D.. Simon, Children's Hospital Los Angeles, Los Angeles, CA, United States; Christopher John. Russell, Stanford University School of Medicine, Palo Alto, CA, United States
Assistant Professor Johns Hopkins All Children's Hospital Saint Petersburg, Florida, United States
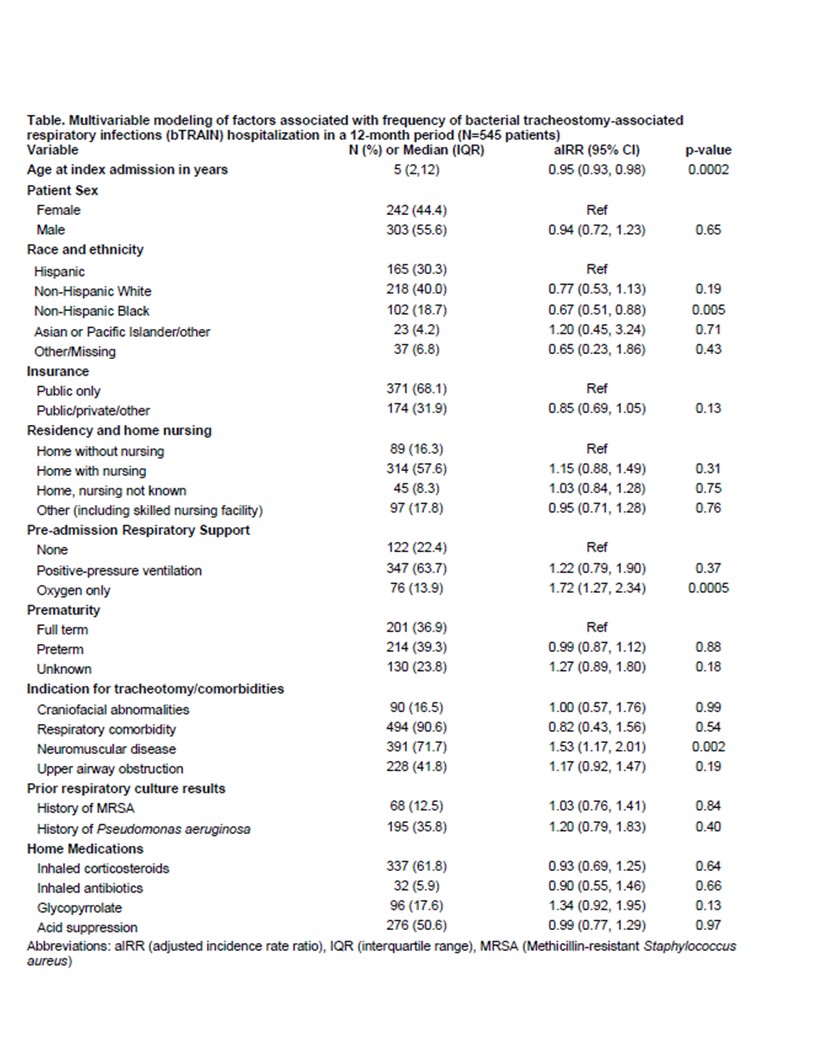
Background: Children with tracheostomy are frequently hospitalized with bacterial tracheostomy-associated infections (bTRAINs; e.g., pneumonia, tracheitis). Efforts to reduce the burden of hospitalization on patients and families are hindered by limited understanding of which patient and clinical features lead to recurrent hospitalizations. Objective: Identify factors associated with recurrent bTRAIN hospitalizations over a 12-month period. Design/Methods: We conducted a multicenter, prospective cohort study of children with pre-existing tracheostomy hospitalized for bTRAIN at one of six freestanding children's hospitals from 2020-2024. Our primary outcome was the number of bTRAIN hospitalizations (defined as respiratory culture obtained, discharge bTRAIN diagnosis, and receipt of complete antibiotic treatment course documented by discharging physician) within 12 months following discharge from the index bTRAIN hospitalization. Children with any hospitalization >37 days, or patients known to leave the health system during follow-up were excluded. We used a multivariable mixed effects negative binomial regression model with a random effect for site to identify independent associations between patient demographic and clinical factors and our primary outcome. Effect sizes are provided as adjusted incident rate ratios (aIRR) and 95% confidence intervals (95% CI). Results: Of the 545 children included, 44% were female, 68% had public insurance, and 30% were Hispanic ethnicity (Table). Median age at index hospitalization was 5 years [IQR 2-12 years]. Children frequently used home mechanical ventilation (HMV; 64%) and had concomitant neuromuscular disease (72%). Overall, 36% of children had at least one additional bTRAIN hospitalization during the follow-up period (range: 0-7). Recurrent hospitalization was associated with comorbid neuromuscular disease (aIRR 1.53 [95% CI 1.17-2.01]). Also, those using home oxygen without HMV had higher number of hospitalizations compared to patients not receiving home respiratory support (aIRR 1.72 [95% CI 1.27-2.34. Older age (aIRR 0.95 [95% CI 0.93-0.98]) and Non-Hispanic Black race and ethnicity (aIRR 0.67 [95% CI 0.51-0.88] were associated with less frequent hospitalization.
Conclusion(s): Children with neuromuscular disease and receiving supplemental oxygen without HMV experience recurrent bTRAIN hospitalizations. Future studies investigating other modifiable factors (i.e., home care practices) and the pathobiology of bTRAIN infections in recurrent hospitalization are warranted.

 photo")