Session: Medical Education 1: Diversity, Equity, and Inclusion
259 - Building Comfort in the Uncomfortable: Creation of a Simulation Based Communication Curriculum to Address Microaggressions in the Clinical Learning Environment
Friday, April 24, 2026
5:30pm - 8:00pm ET
Publication Number: 1245.259
Olivia O. Familusi, Children's Hospital of Philadelphia, Philadelphia, PA, United States; Nicole R. Washington, Children's Hospital of Philadelphia, Philadelphia, PA, United States; Ashley E. Martin, The Chi, Philadelphia, PA, United States; Ashley Bach, Childrens Hospital of Philadelphia, Philadelphia, PA, United States; Sophie Lieberman, Childrens Hospital of Philadelphia, Philadelphia, PA, United States; Josh Kurtz, Children's Hospital of Philadelphia, Philadelphia, PA, United States; Tara Bamat, CHOP, Philadelphia, PA, United States
Pediatric Hospital Medicine Fellow Children's Hospital of Philadelphia Philadelphia, Pennsylvania, United States
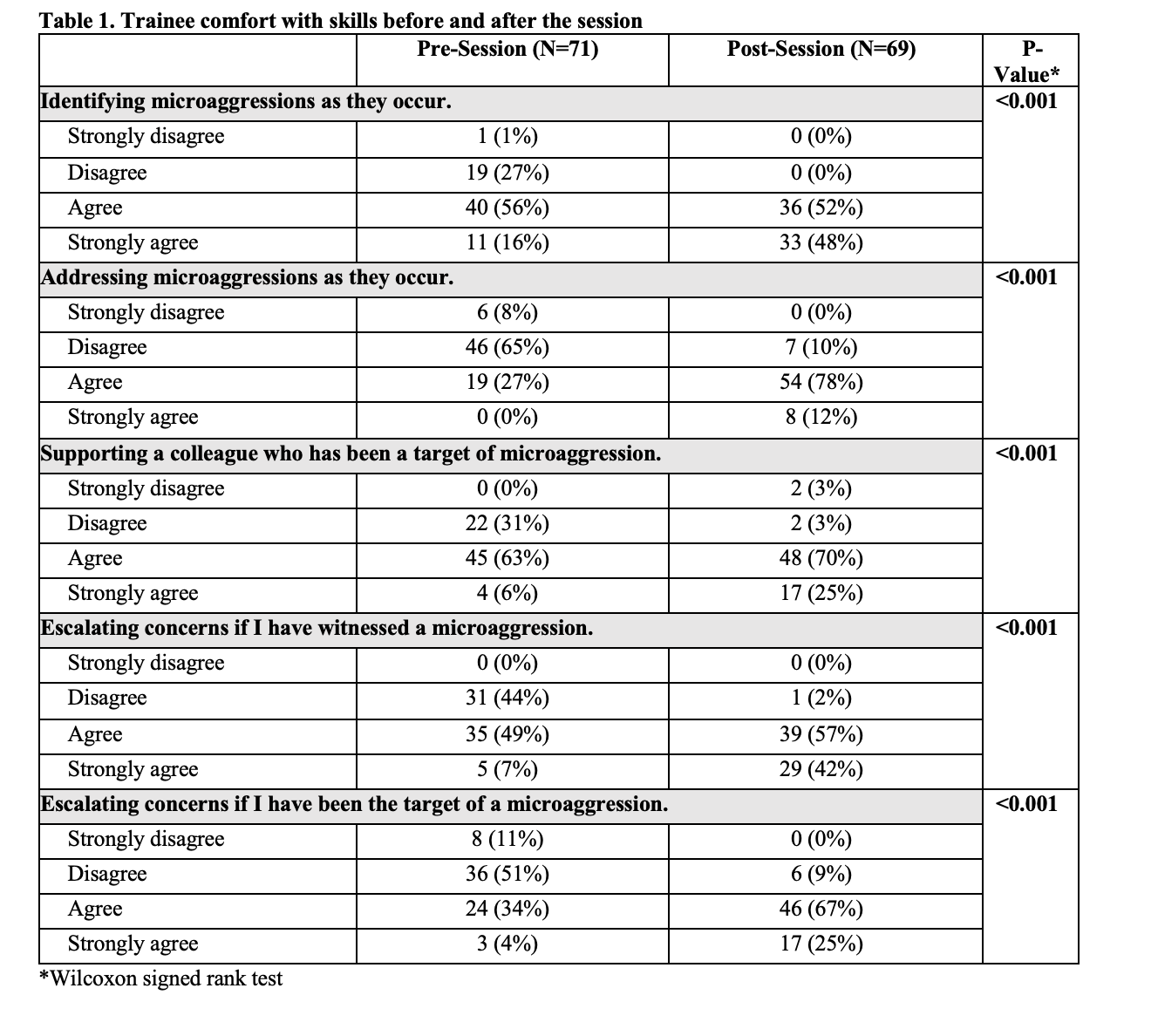
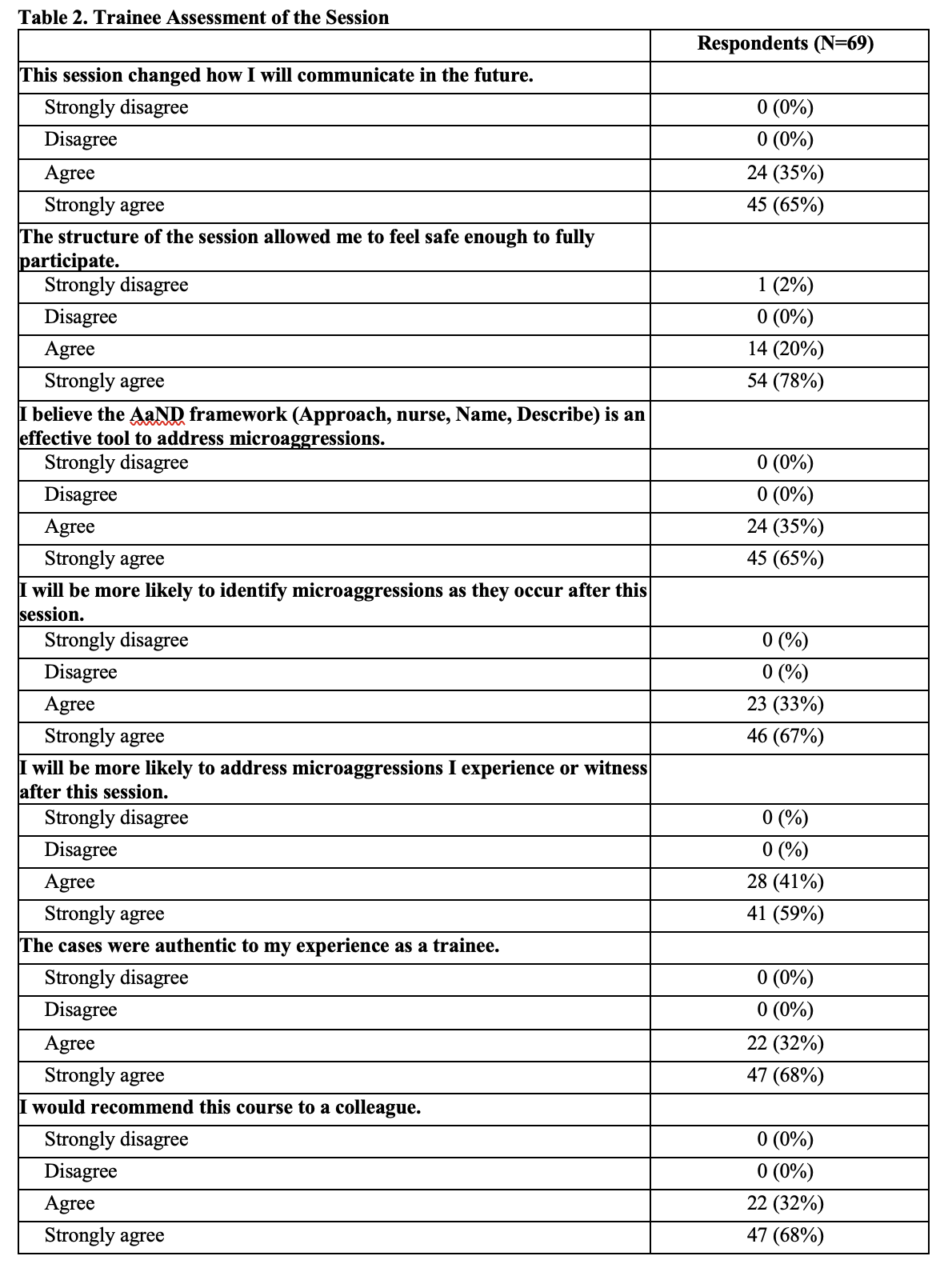
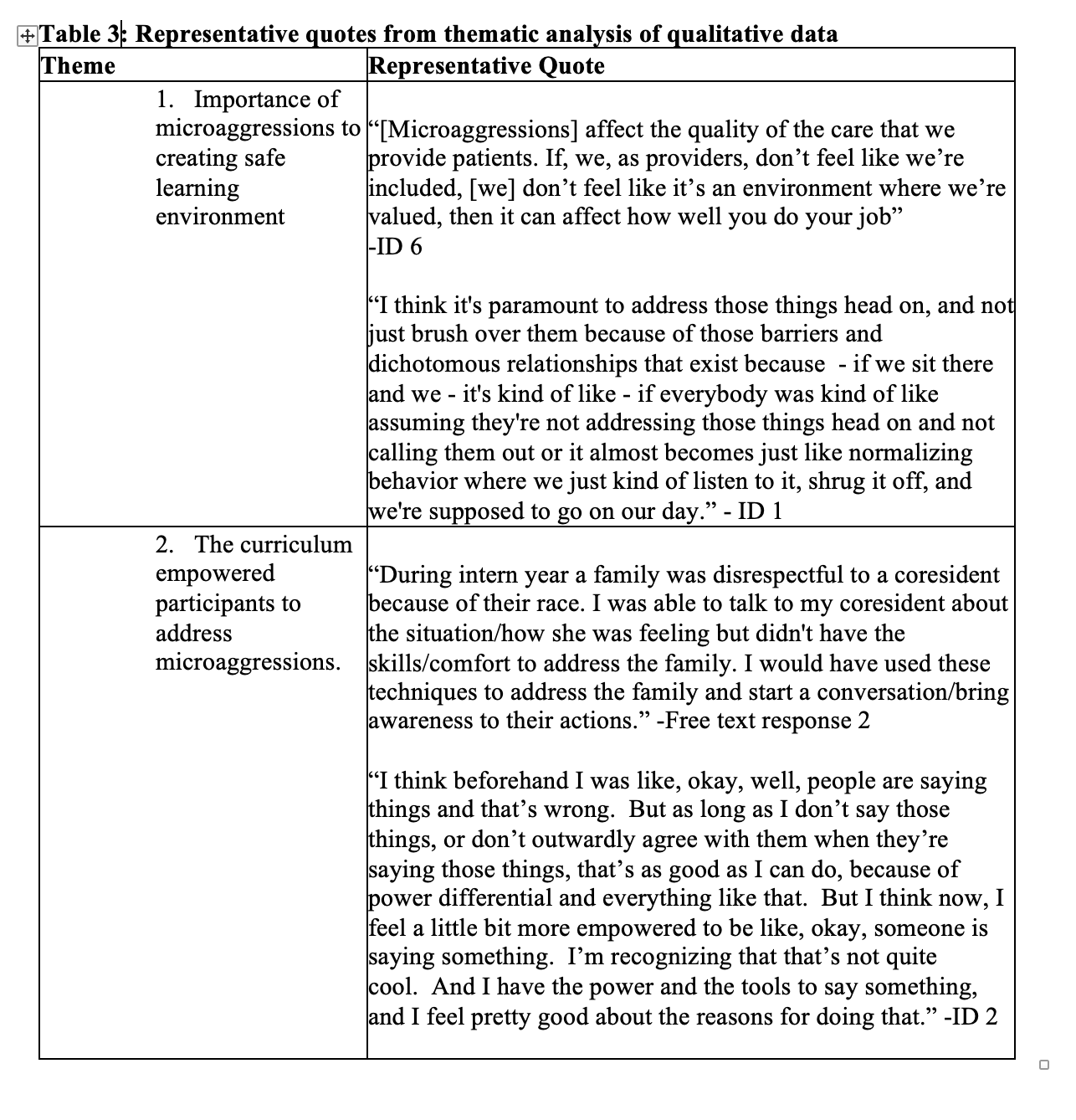
Background: Microaggressions in the clinical learning environment occur frequently and contribute to trainee burnout. Neither trainees nor faculty report feeling equipped to respond to microaggressions. While microaggressions curricula exist, there is a gap in curricula focused on direct skill-building in identifying, navigating the power dynamics of, and directly addressing microaggressions. Objective: We aimed to develop and implement a psychologically safe simulation session that teaches residents to identify, discuss power dynamics of, and directly address microaggressions in the clinical learning environment using VitalTALK, a validated communication simulation methodology that underscores the importance of emotional tracking during difficult conversations. Design/Methods: Between 2021-2024, PGY-3 and 4 pediatrics residents completed a 4-hour-long simulation-based session on microaggressions using VitalTalk methodology. The intervention was led by trained VitalTalk facilitators, bias and equity educators, and patient actors. All participants were invited to complete anonymous pre- and post-session surveys. One-on-one interviews were conducted to further assess self-perceived comfort with microaggressions. Descriptive statistics were used to summarize quantitative data and Wilcoxon Signed Rank test was used to compare Likert-scale responses before and after the sessions. Qualitative data was analyzed via template analysis approach. Results: 71 residents completed the pre-session survey, and 69 (97%) completed the post-session survey. 11 interviews were completed. From survey results, residents' perceived comfort identifying and addressing microaggressions increased significantly after the session. Qualitative data showed that residents agreed that the session's framework was effective, that they felt safe enough to participate, and that they felt empowered to identify or address microaggressions following the session.
Conclusion(s): Our novel VitalTalk Microaggressions course improves trainee comfort with identifying and addressing microaggressions. Future directions include assessing longitudinal behavioral change associated with this innovative intervention.
Trainee comfort with skills before and after the session
Table 2. Trainee Assessment of the Session
Table 3: Representative quotes from thematic analysis of qualitative data