598 - An Interdisciplinary Quality Improvement Initiative to Improve Inpatient Boarding in the Pediatric Emergency Department
Friday, April 24, 2026
5:30pm - 8:00pm ET
Publication Number: 1575.598
Divya Lakhaney, Columbia University Irving Medical Center, New York, NY, United States; Katherine Ryan, Boston Children's Hospital, Boston, MA, United States; Laurie Malia, Columbia University Vagelos College of Physicians and Surgeons, New York, NY, United States; Christie Parrett, NewYork-Presbyterian Morgan Stanley Children's Hospital, New York, NY, United States; Katherine Schlosser Metitiri, NewYork-Presbyterian Morgan Stanley Children's Hospital, New York, NY, United States; Tammy Compagnone, NewYork-Presbyterian Morgan Stanley Children's Hospital, New York, NY, United States; Czer Anthoney E. Lim, Columbia University Vagelos College of Physicians and Surgeons, New York, NY, United States
Division Chief, Pediatric Emergency Medicine Columbia University Vagelos College of Physicians and Surgeons New York, New York, United States
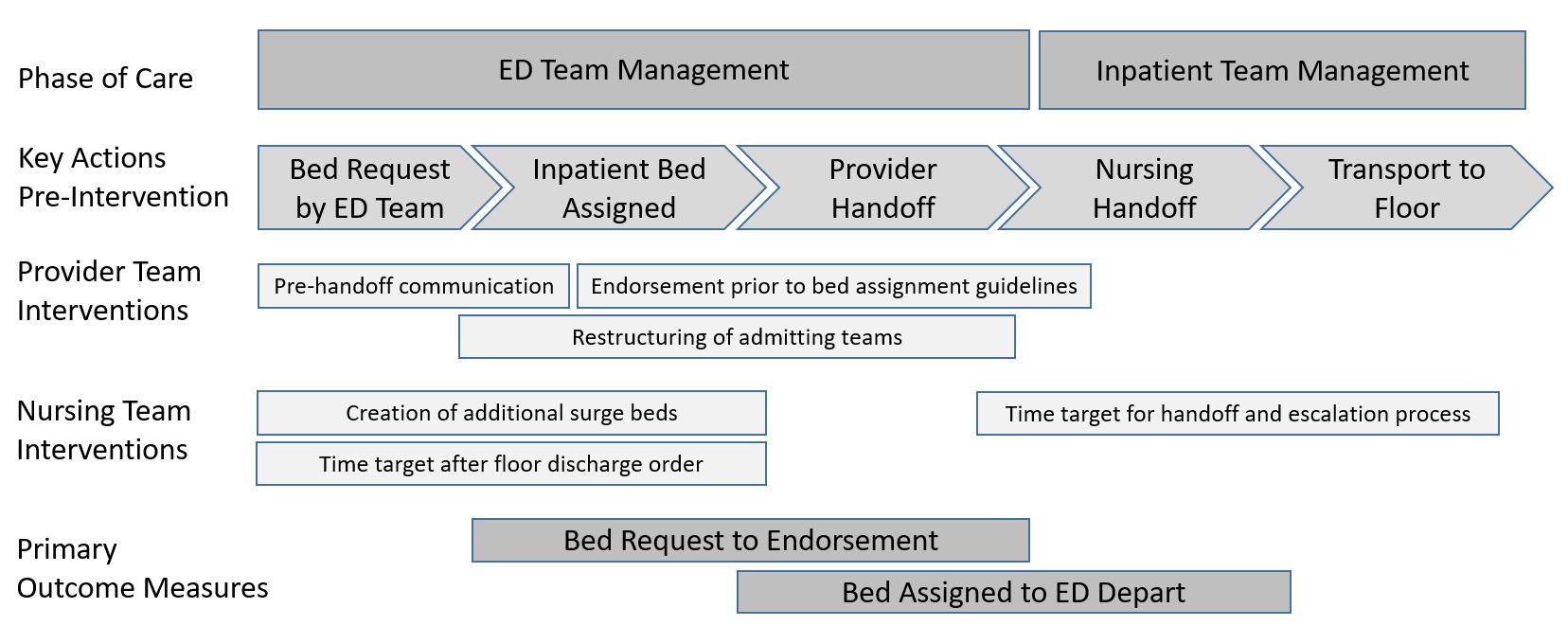
Background: Emergency Department (ED) boarding is the practice of holding patients in the ED after a decision to admit has been made, typically due to a lack of available inpatient beds. The aim of this project was to advance the care of patients in the ED requiring admission by improving the transition of care to inpatient teams. Objective: Our quality improvement (QI) aims were to decrease the times from 1) admit decision to handoff to inpatient teams (endorsement) and 2) from bed assignment to ED departure. Design/Methods: At our urban, academic, children's hospital, we formed an interdisciplinary QI team consisting of inpatient, ED, nursing, and hospital stakeholders. A process map was created outlining the workflow from bed request to patient transfer to the inpatient unit and targeted interventions were implemented. These included early communication regarding admissions, implementation of guidelines identifying patients that can be handed off to inpatient teams while awaiting bed assignment, restructuring of inpatient teams to increase admitting capacity, establishment of time expectations on nursing handoff, and creation of additional treatment spaces (Fig 1).
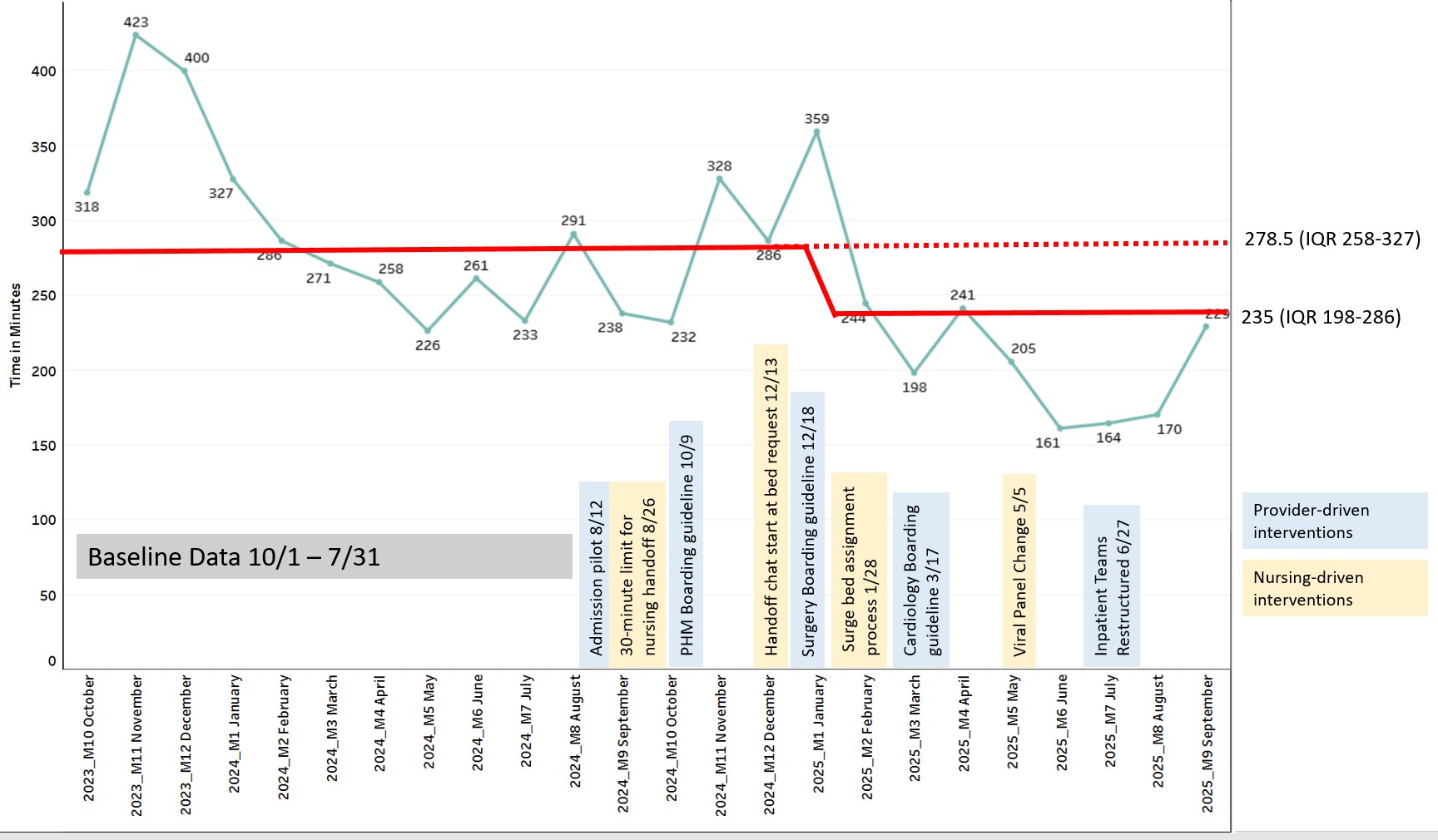
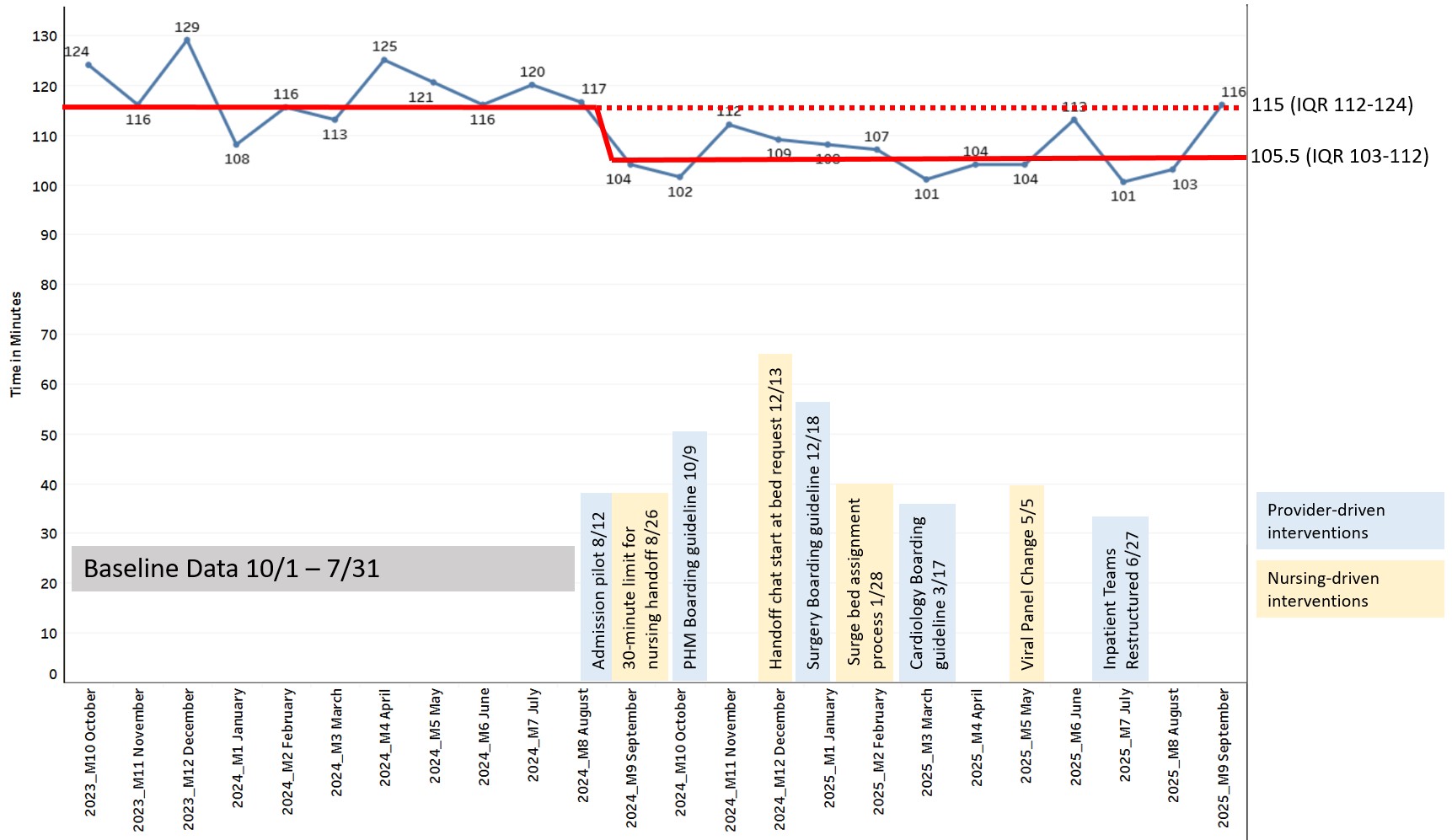
Interventions employed a Plan Do Study Act methodology and the QI team met bi-weekly to review and analyze statistical process control charts to make iterative changes to subsequent cycles. Primary outcome measures included time from bed request to endorsement and time from bed assignment to ED departure. Balancing measures include ED length of stay (LOS) and change in level of care following endorsement. Results: From October 2023 to September 2025, there were 109,087 ED visits and 12,802 admission (11.7%). 5,762 (45%) admissions occurred during the pre-implementation period and 7,040 (55%) occurred during the implementation period which began in August 2024. The median time from bed request to endorsement decreased by 43.5 minutes (15.6%) and time from bed assignment to ED depart decreased by 9.5 minutes (8.2%). Statistical process control chart sustained a centerline shift for both outcomes (Fig 2 and 3). There was a 54.9% increase in number of patients endorsed prior to bed assignment. There was no change in the median ED LOS of 3.1 hours (2.9-3.1). 5 patients required change in level of care following endorsement. Over the implementation period, 5,104 hours of ED provider care and 1,114 hours of ED nursing care were saved.
Conclusion(s): In this ongoing work, an interdisciplinary quality improvement team was able to significantly improve throughput efficiency for patients requiring admission from the ED at our children's hospital.
Figure 1: Process map, description of interventions and primary outcome measures
Figure 2: Statistical process control chart for time from bed request to endorsement by interventions
Figure 3: Statistical process control chart for time from bed assignment to ED departure by interventions

 Credit")