782 - Reduction in Severe Intraventricular Hemorrhage Following Implementation of a Small Baby Program: A Tertiary NICU Quality Improvement Study
Friday, April 24, 2026
5:30pm - 8:00pm ET
Publication Number: 1758.782
Alence E. Zion, Northeastern University, Boston, MA, United States; Margaret F. Everett, Harvard Medical School, Boston, MA, United States; Channing S. Pooley, Tufts University School of Medicine, Charlestown, MA, United States; Ceilidh Smith, Brigham and Women's Hospital, Boston, MA, United States; Hoda El-Shibiny, Brigham's Women Hospital, Boston, MA, United States; Danielle Ben-David, Brigham and Women’s Hospital, Boston, MA, United States; Laura B. Bernardini, Brigham and Women's Hospital and Harvard Medical School, Boston, MA, United States; Elizabeth Brennick, Brigham and Women's Hospital, Boston, MA, United States; Elisabeth Kaza, Brigham and Women's Hospital, CHESTNUT HILL, MA, United States; Stephanie Neville, Brigham and Women's Hospital, Stoneham, MA, United States; Kendra Woo, Brigham and Women's Hospital NICU, Boston, MA, United States; Julie Cadogan, Brigham and Women's Hospital, Boston, MA, United States; Elisa Abdulhayoglu, Brigham & Women's Hospital, Lynnifeld, MA, United States; Elizabeth Y. Flanigan, Elizabeth, Westford, MA, United States; Mohamed El-Dib, Brigham and Women's Hospital / Harvard Medical School, Boston, MA, United States
Student Northeastern University Boston, Massachusetts, United States
Background:
Background: Germinal matrix - intraventricular hemorrhage (GM/IVH) is a brain injury in preterm infants that may lead to neurodevelopmental delays, and increased mortality. IVH is classified: Grades I and II are mild IVH while Grades III and IV are severe IVH (SIVH). Babies born < 28 weeks have increased risk of GM/IVH, increasing as GA decreases. Objective: Problem Statement: At BWH from 2019 to September of 2021, of 109 babies born at gestation less than 28 weeks, 50 (48%) babies developed IVH; 22 (20%) grades I-II and 28 (26%) grades III-IV.
SMART
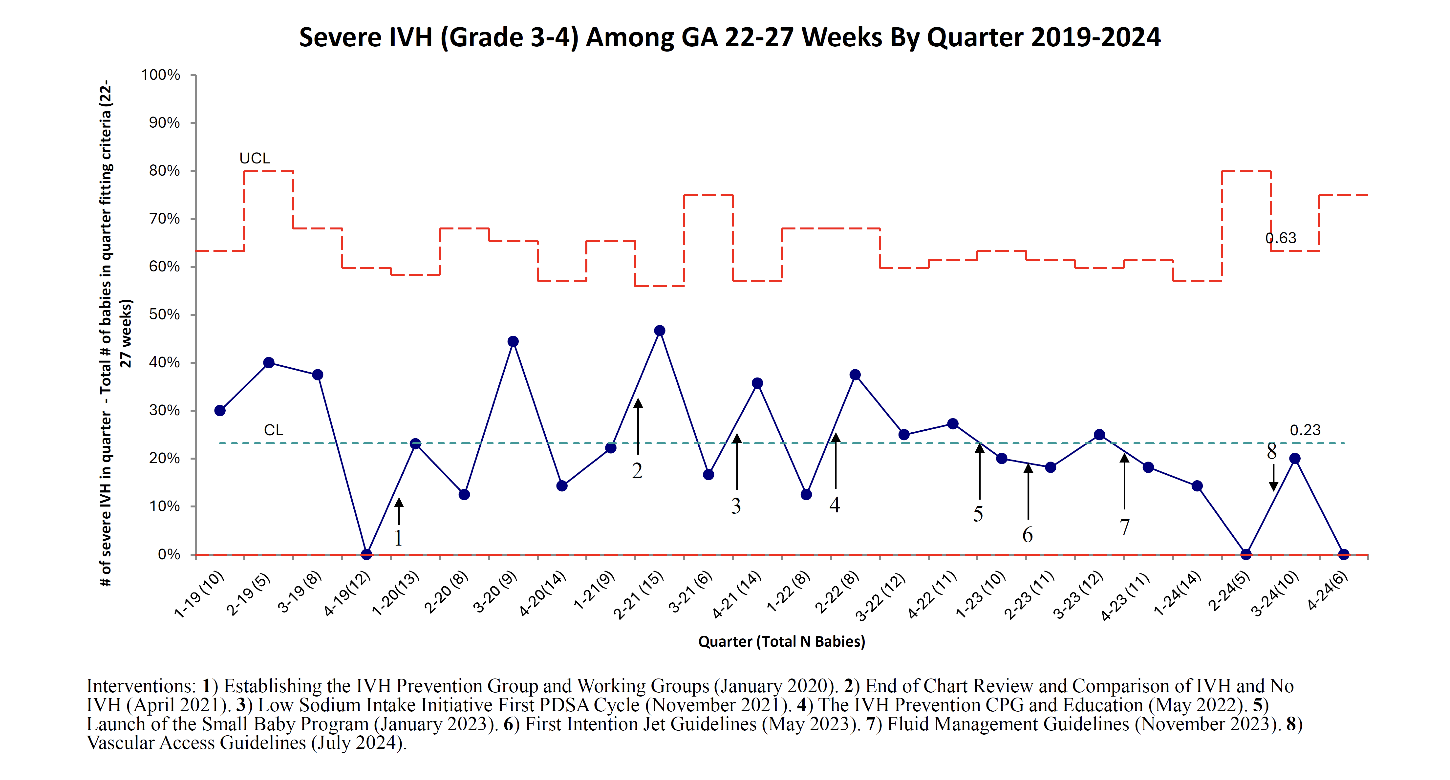
Aim: To reduce the rate of SIVH in infants born less than 28 weeks' gestation at Brigham and Women's Hospital (BWH) by 30% over 3 years starting October 2021, using targeted neuroprotective strategies. Design/Methods: Methods: Baseline data at BWH was collected from January 2019 through September 2021. Data was obtained from BWH NICU Vermont Oxford Network (VON), using VON definitions. The electronic medical record (EMR) was used to complete missing data. A driver diagram was created to choose interventions for the Multiple Plan-Do-Study-Act (PDSA) cycles used to implement and evaluate change. Changes in rates of IVH were monitored from October 2021 to December 2024.
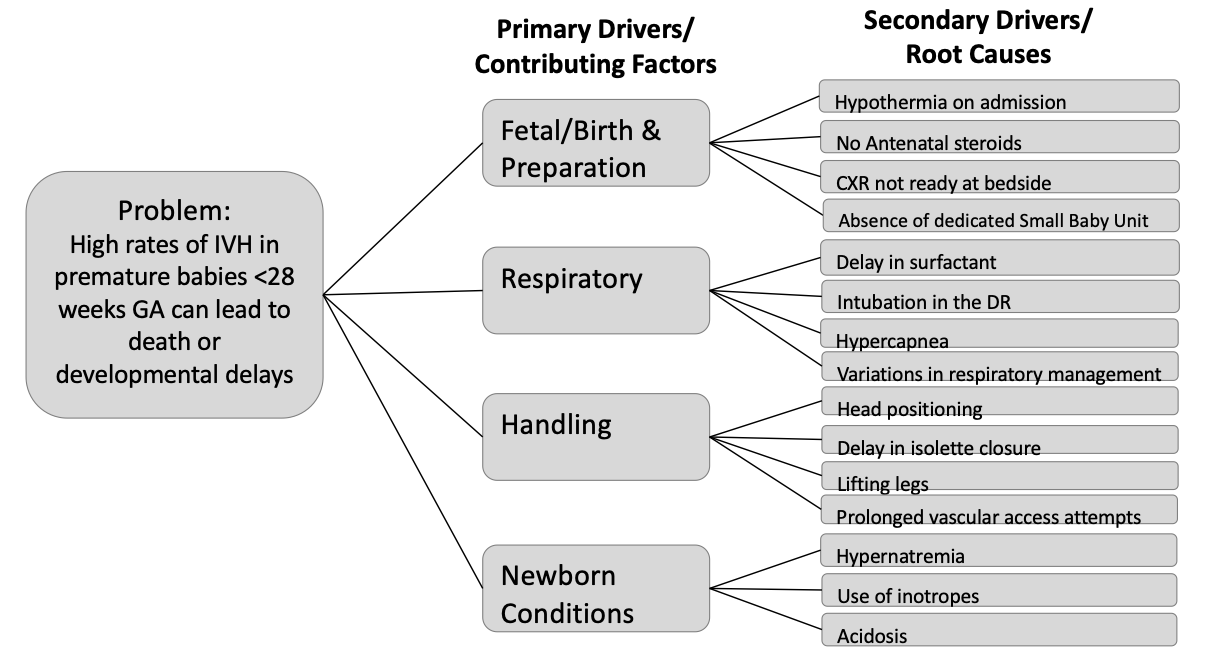
Interventions: A multidisciplinary IVH Reduction Task Force and the Small Baby Program were established and launched variable interventions. These interventions include the Low Sodium Intake Initiative, IVH Prevention Clinical Practice Guideline, First Intention Jet Guidelines, Fluid Management Guidelines and Vascular Access Guidelines, which support neuroprotective care practices. Results: Over the intervention period, 132 babies were born with a gestational age of less than 28 weeks GA. Table 1 compares the basic demographic and clinical characteristics of infants in the baseline period and intervention period. Figure 1 shows the primary and secondary drivers evaluated as contributors to IVH development. Figure 2 shows a Control chart representing SIVH rate over the study period. In 2024, although 57% of the infants were reported to have any IVH; the rate of SIVH was 11% (more than 50% reduction of baseline).
Conclusion(s): While there is no QI Special Cause Variation in SIVH, early trends suggest that a structured QI approach may support reductions in SIVH over time. A Small Baby Program initiative can assist with neuroprotective efforts and has the potential to reduce the risk of severe IVH.
Table 1: Demographic and Clinical Data of the Study Cohort

 Credit")
.png)