628 - Beyond the Threshold: Maternal Glucose Values and Adverse Neonatal Outcomes in the Absence of a Gestational Diabetes Mellitus Diagnosis
Friday, April 24, 2026
5:30pm - 8:00pm ET
Publication Number: 1605.628
Reshma Silas, Hassenfeld Children's Hospital at NYU Langone, Jersey City, NJ, United States; Heather Howell, New York University Grossman School of Medicine, New York, NY, United States; Kelsy Miranda, New York University Grossman School of Medicine, New York, NY, United States; Noha Nizam, State University of New York Downstate Medical Center College of Medicine, Richmond Hill, NY, United States; Amy Sarker, Hassenfeld Children's Hospital at NYU Langone, Jackson Heights, NY, United States; Robert Angert, New York University Grossman School of Medicine, NEW YORK, NY, United States
Undergraduate Student New York University Grossman School of Medicine Brewster, New York, United States
Background: Gestational Diabetes Mellitus (GDM) affects approximately 5-15% of pregnancies in the United States with infants of GDM mothers at risk of large-for-gestational-age (LGA) , macrosomia, and hypoglycemia. At NYU Langone Health, GDM is screened by the Carpenter-Coustan 2-step method, a 50 g glucose challenge test (GCT) followed by a glucose tolerance test (GTT) if abnormal. However, infants of women who screen negative may still experience complications, suggesting that the current approach may fail to identify some at-risk pregnancies. Objective: To describe infants admitted to the NICU for, LGA, macrosomia or hypoglycemia whose mothers screened negative for GDM, and compare neonatal outcomes across levels of maternal dysglycemia. Design/Methods: This was an IRB-exempt, single-center retrospective chart review. Eligible neonates were ≥37 weeks' GA, admitted to the NICU between January 1, 2023, to June 1, 2025, for LGA, macrosomia or hypoglycemia. Maternal screening results were categorized into four groups of increasing dysglycemia: (1) normal GCT, (2) abnormal GCT with normal GTT, (3) abnormal GCT with 1 abnormal GTT value, and (4) GDM (≥2 abnormal GTT values). Statistical analyses included ANOVA and chi-square testing with significance at p < 0.05. Results: Of the eligible 11,680 neonates ≥37 weeks, 1,214 were admitted to the NICU and 310 met criteria. After exclusions, 249 neonates remained: Group 1 (65.1%, n=162), Group 2 (18.1%, n=45), Group 3 (4.4%, n=11), Group 4 (12.4%, n=31). Overall rate of NICU admissions for the combined characteristics of LGA, macrosomia and hypoglycemia (Groups 1-4) was 2.1% (249/11,680). Assuming the standardized global prevalence of GDM at 14% the estimated population of pregnancies with negative screen is 10,014 and screen positive is 1,635. For those with negative GDM screening (Groups 1-3) the estimated NICU admission rate is 2.2% (≈218/10,014). For those with positive GDM screening (Group 4), the estimated rate was 1.9% (31/1,635).
Conclusion(s): GDM screening led to the identification of infants at risk for complications with combined screening and interventions resulting in a neonatal admission rate of 2.2%. Maternal dysglycemia within the non-diagnostic range for GDM was associated with adverse neonatal outcomes highlighting the need for close monitoring and targeted interventions in these patients. Larger studies are needed to validate these findings and ensure generalizability. We also plan to study neonates not admitted to the NICU to better assess the performance of the screening test and impact of subsequent interventions.
Maternal Groups by Increasing Dysglycemia Figure 1

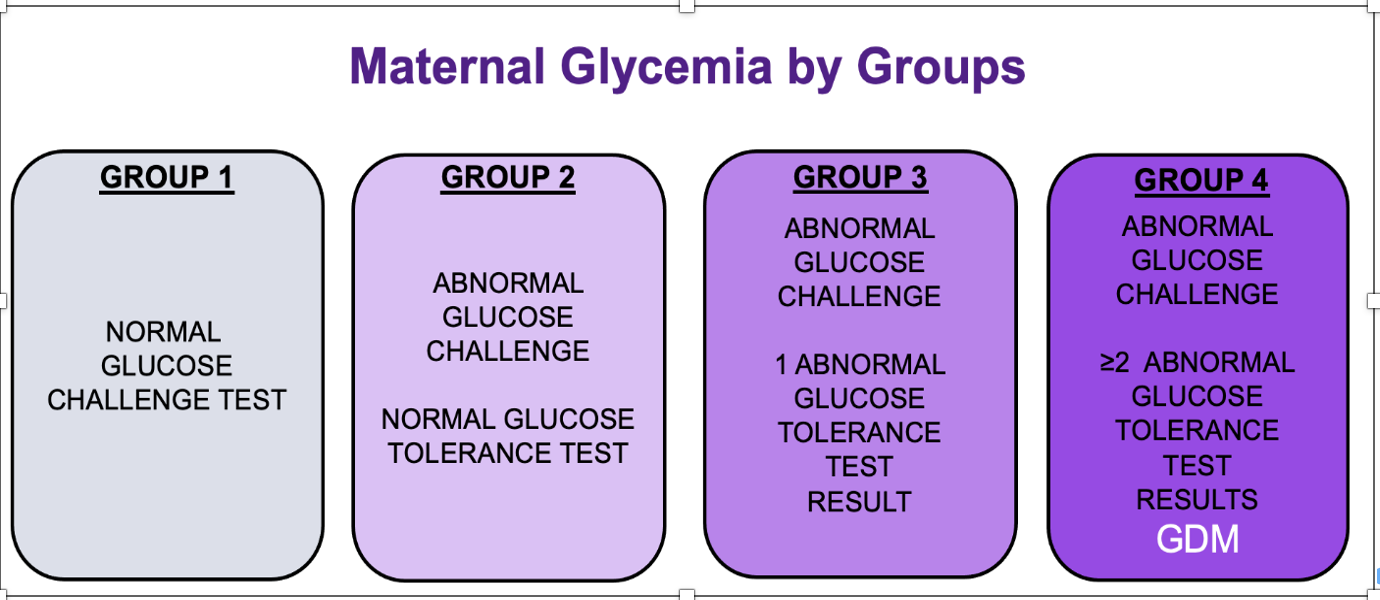 Figure 1
Figure 1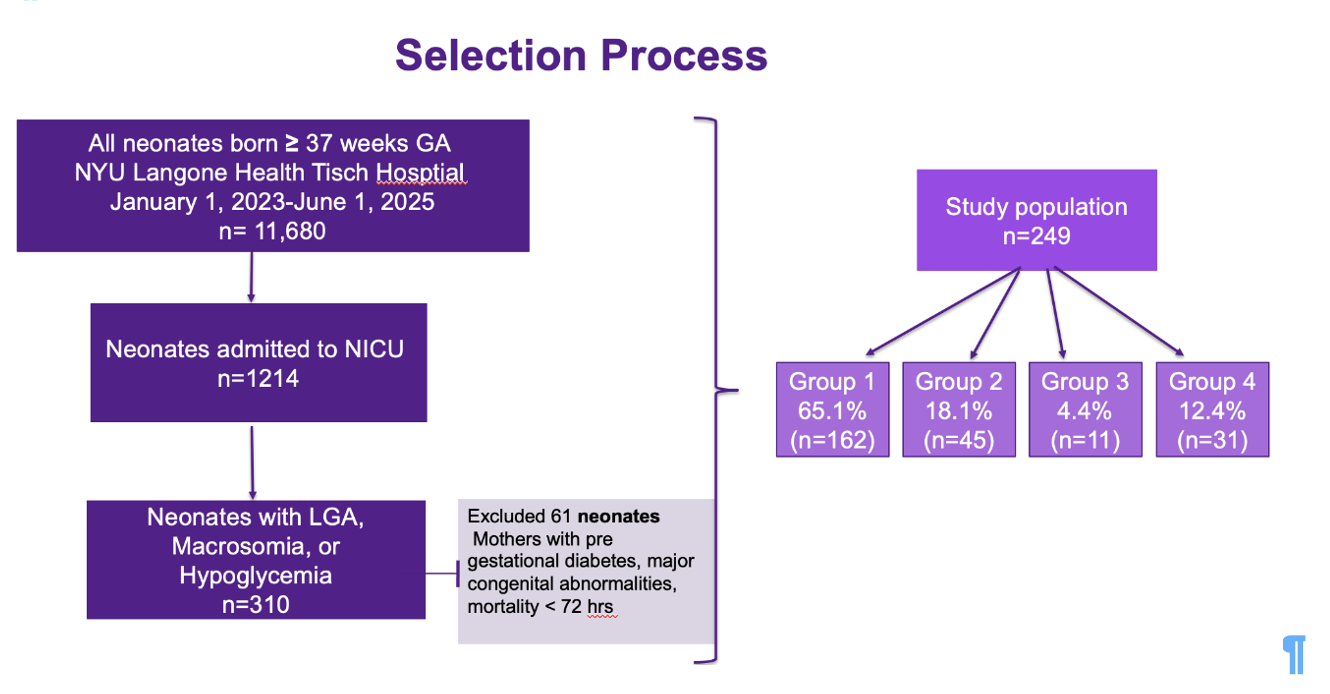 Figure 2
Figure 2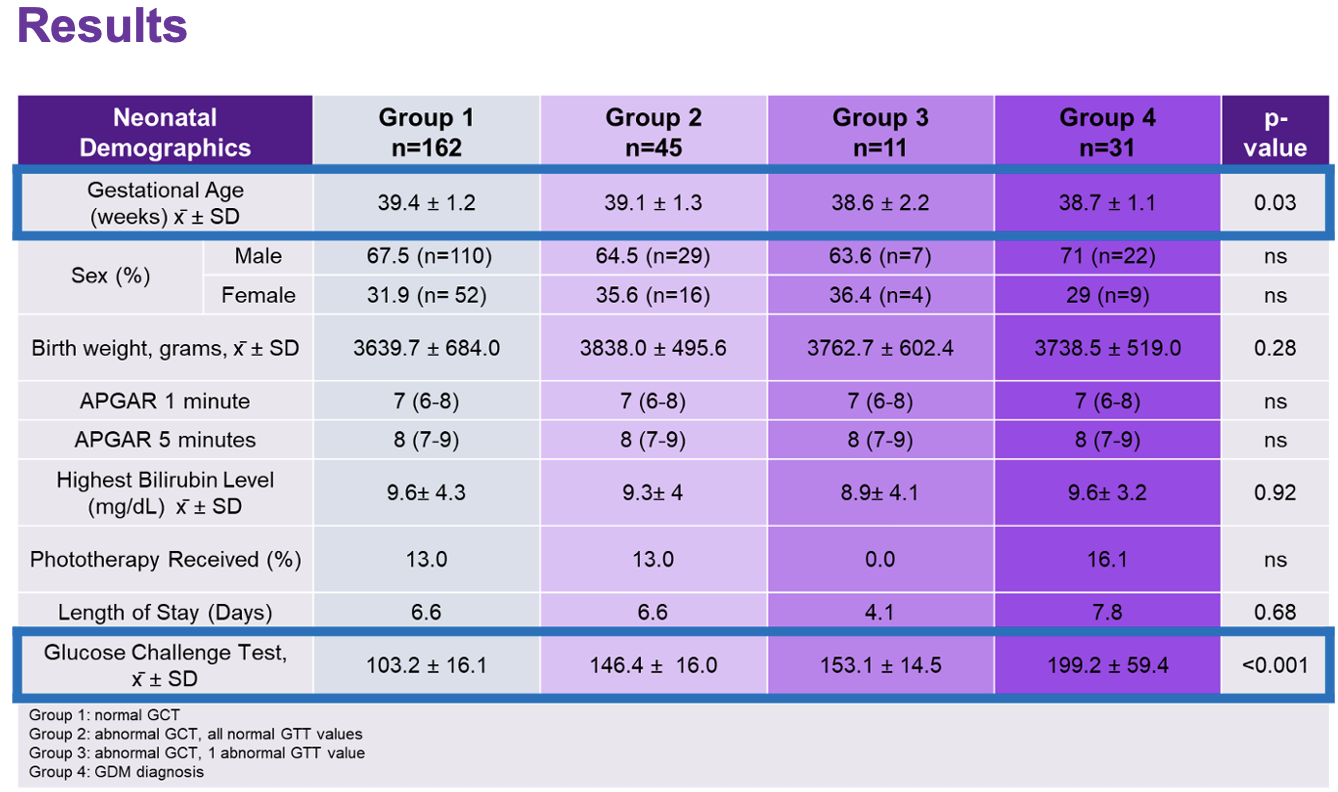 Table 1
Table 1