28 - Cooling in mild encephalopathy (COMET) pilot randomised trial: neurodevelopmental outcomes at two years
Friday, April 24, 2026
5:30pm - 8:00pm ET
Publication Number: 1025.28
Paolo Montaldo, Imperial College London, lONDON, England, United Kingdom; Reema Garegrat, Imperial College London, London, England, United Kingdom; Simona Puzone, University of Campania Luigi Vanvitelli, Naples, Campania, Italy; Anchal Dhawan, Imperial College London, London, England, United Kingdom; Mia Cunliffe, Imperial College London, London, England, United Kingdom; Stuti Pant, Imperial College London, London, England, United Kingdom; Thilipan Thaventhiran, Imperial College London, LONDON, England, United Kingdom; Palaniappan Sashikumar, Medway Maritime Hospital, Gillingham, England, United Kingdom; Santosh Pattnayak, Medway Maritime Hospital, Gillingham, England, United Kingdom; Aung Soe, Medway Hospital, Gillingham, England, United Kingdom; Sundeep Harigopal, Newcastle Upon Tyne NHS Foundation Trust, Newcastle upon Tyne, England, United Kingdom; Balamurugan Palanisami, n, Liverpool, England, United Kingdom; Narendra Aladangady, NHS, London, England, United Kingdom; Seetha Shankaran, University of Texas at Austin Dell Medical School, Ann Arbor, MI, United States; Sudhin Thayyil, Imperial College London, London, England, United Kingdom
Research Fellow Imperial College London lONDON, England, United Kingdom
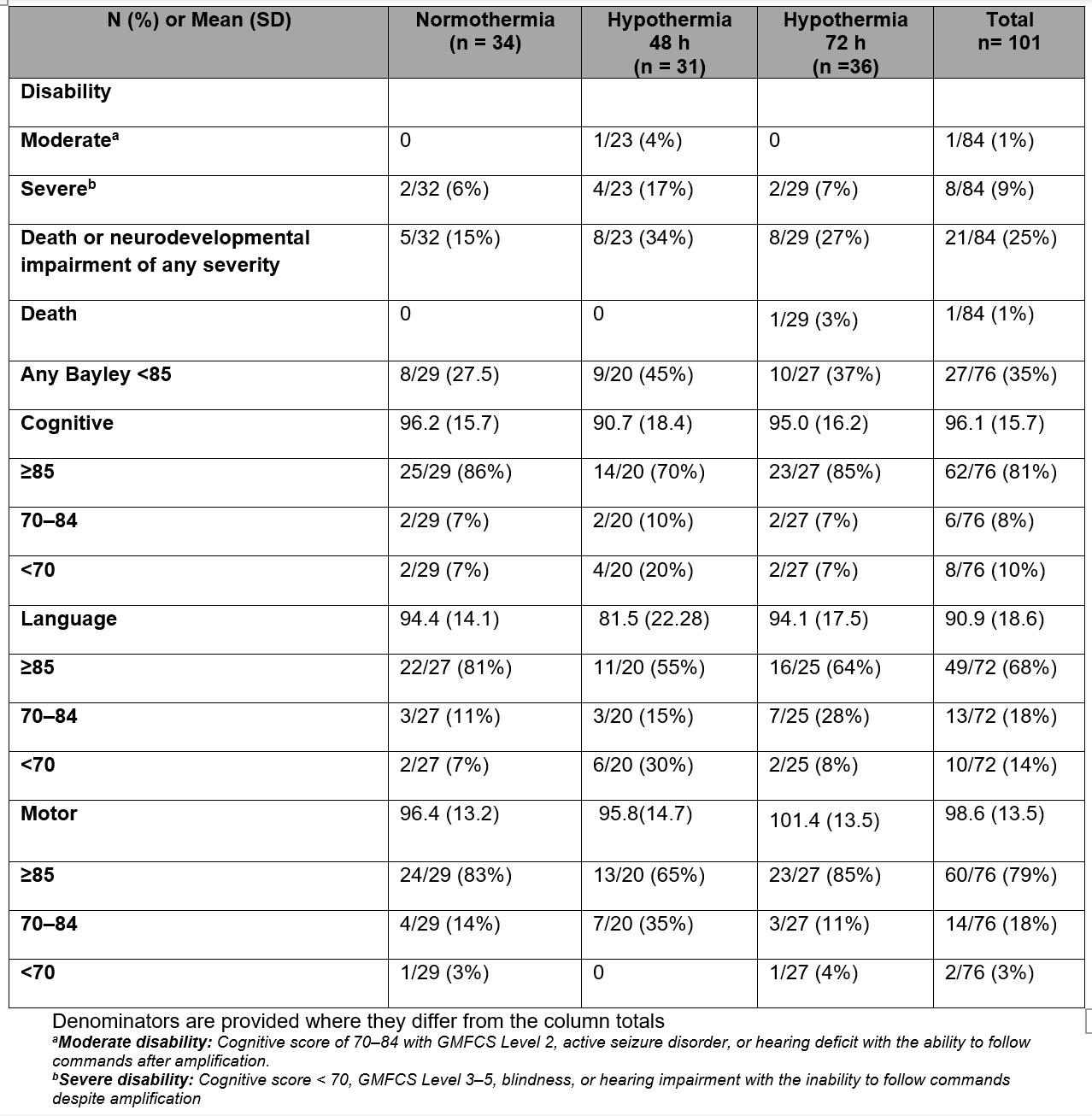
Background: Although induced hypothermia benefits moderate to severe HIE, its safety in mild HIE has not been evaluated. Objective: We report two-year neurological outcomes from a pilot trial comparing normothermia with 48 hours and 72-hour whole-body hypothermia in mild HIE. Design/Methods: The pilot RCT enrolled 101 infants born at or after 36 weeks with severe birth acidosis or birth depression and mild HIE, classified using the Expanded modified Sarnat staging by trained, certified examiners across six sites in the UK and Italy. Infants aged < 6 hours were randomised to normothermia or whole-body hypothermia for 72 hours (Group A; n=48). Those aged >6 hours and already receiving induced hypothermia were randomised to rewarming at either 48 or 72 hours (Group B; n=53). Thus 34 infants were in normothermia, 31 had 48h and 36 had 72 h hypothermia. Neurodevelopmental outcomes were assessed at two years using the Bayley IV scales of infant development, masked to group allocation, or by, the Parent Report of Children's Abilities - Revised (PARCA-R) questionnaire if Bayley assessment could not be performed. Adverse outcome was defined as death or any neurodevelopmental impairment (Gross Motor Function Classification System (GMFCS) level ≥1 or cognitive score < 90). Results: Outcome data at 2 years were available from 84 out of 101 (83%) of recruited infants (94% in Group A and 75% in Group B) Of these, Bayley IV was performed in 76/84 (90%) and PARCA-R in 8/84 (10%). Overall adverse outcomes occurred in 21 (25%) - normothermia 5 (15%), 48 h hypothermia 8 (34%) and 72 hour hypothermia 8 (27%) Moderate disability occurred in 1 child (1%) part of the 48 h hypothermia group. Severe disability (including cerebral palsy and autism) occurred in in 8 (9%) - normothermia 2 (6%), 48 h hypothermia 4 (17%) and 72-hour hypothermia 2 (7%) (Table 1, Figure 1).
Conclusion(s): Adverse outcomes occurred in 25% of the babies with mild HIE, of which (8%) have severe disability. Safety and efficacy of whole-body hypothermia need to be examined in an adequately powered randomised controlled trial before it is offered as standard clinical care.
Table 1. Neurodevelopmental outcomes in the normothermia and whole-body hypothermia groups.
Figure 1. Box plots (median, IQR) of the neurodevelopmental outcome scores in the different groups . WBH: Whole-body hypothermia.

 photo")
.png) WBH: Whole-body hypothermia.
WBH: Whole-body hypothermia.