552 - Prolonged Infusion vs Standard Bolus Meropenem in Critically Ill Pediatric ICU Patients With Sepsis: A Randomized Clinical Trial
Friday, April 24, 2026
5:30pm - 8:00pm ET
Publication Number: 1531.552
Samar Elassar, Flushing Hospital Medical Center, New york, NY, United States; Muhammad Abdullah, Bahria university health Sciences Campus Karachi, Karachi, Sindh, Pakistan; Rida Shakeel, Dow Medical College, Karachi, Karachi, Sindh, Pakistan; Dalia Atef Abouda, Faculty of medicine Alexandria University Egypt, Beheria, Abu Matamir, Al Buhayrah, Egypt; Aleena Ihtasham, King Edward Medical University, Lahore, Punjab, Pakistan; Sana Munir, Mohtarma Benazir Bhutto Shaheed Medical College Mirpur AJK Pakistan, Mirpur, Azad Kashmir, Pakistan; Wissal Fatih, caddi ayad university, Marrakech, Marrakech-Tensift-Al Haouz, Morocco
Resident Alexandria university faculty of medicine New york, New York, United States
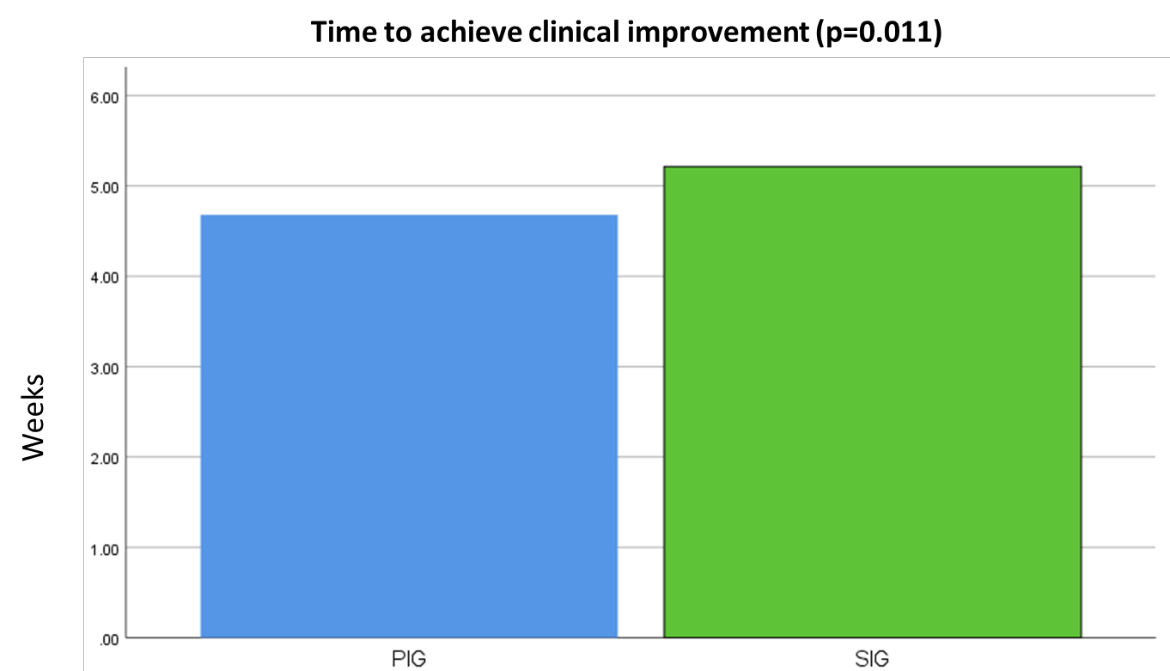
Background: Critically ill children with sepsis in the pediatric ICU face high morbidity due to altered pharmacokinetics and risk of suboptimal antibiotic exposure. Meropenem, a broad-spectrum carbapenem, is commonly used, but standard bolus dosing may fail to maintain concentrations above the MIC for sufficient time. Prolonged infusions optimize time-dependent killing and may improve outcomes, though large pediatric RCTs are scarce. Objective: To compare the efficacy of prolonged 4-hour infusion meropenem (PIG) versus standard 30-minute bolus (SIG) in pediatric ICU patients with sepsis. Design/Methods: This study was conducted in March 2025 at PNS Shifa Hospital in Karachi, Pakistan, and included 150 children aged 1-18 years who had sepsis and were started on meropenem. After receiving ethical approval and parental consent, participants were randomly divided into two equal groups using a computer-generated system: one group received meropenem as a 4-hour extended infusion every 8 hours (n=75; 20 mg/kg per dose), while the other received the same dose over a 30-minute infusion at the same frequency (n=75). Patients with renal impairment or meropenem allergy were excluded. Therapy was administered for a minimum of seven days and extended as clinically indicated. The primary outcome was clinical success, defined as resolution of infection without escalation of antibiotic therapy. Secondary outcomes included microbiologic clearance and time to clinical improvement. Analysis used χ² and t-tests (p < 0.05). Results: Baseline characteristics were balanced between groups. Clinical success was higher with prolonged infusion (92.0% vs 74.7%, p< 0.0001). Microbiologic eradication favored prolonged infusion (85.3% vs 65.3%, p< 0.0001). Time to clinical improvement was shorter (4.7 ± 1.3 vs 5.2 ± 1.2 days, p=0.011). Adverse events did not differ significantly.
Conclusion(s): Prolonged 4-hour meropenem infusion yields superior clinical success, microbiologic clearance, and faster recovery versus standard bolus in critically ill children, supporting its adoption in pediatric ICUs. Broader, multi-center research is needed to support these findings and clarify PK-PD benefits.
Baseline characteristics and Adverse effects
Clinical success rate and Infection clearance rate

.jpg)
.jpg)