673 - Outcome of bloody stools in newborns born < 32 wks gestation evaluated for late onset sepsis in the neonatal intensive care unit.
Friday, April 24, 2026
5:30pm - 8:00pm ET
Publication Number: 1650.673
John Padanilam, Southern Illinois University School of Medicine, Springfield, IL, United States; Mohamed F. Ahamed, Southern Illinois University School of Medicine, springfield, IL, United States; Erin M. Bauer, Southern Illinois University School of Medicine, Springfield, IL, United States; Sean McGinity, Southern Illinois University School of Medicine, Springfield, IL, United States; Beau Batton, Southern Illinois University School of Medicine, Springfield, IL, United States; Venkata S. Majjiga, Physician, Chatham, IL, United States
Resident Southern Illinois University School of Medicine Springfield, Illinois, United States
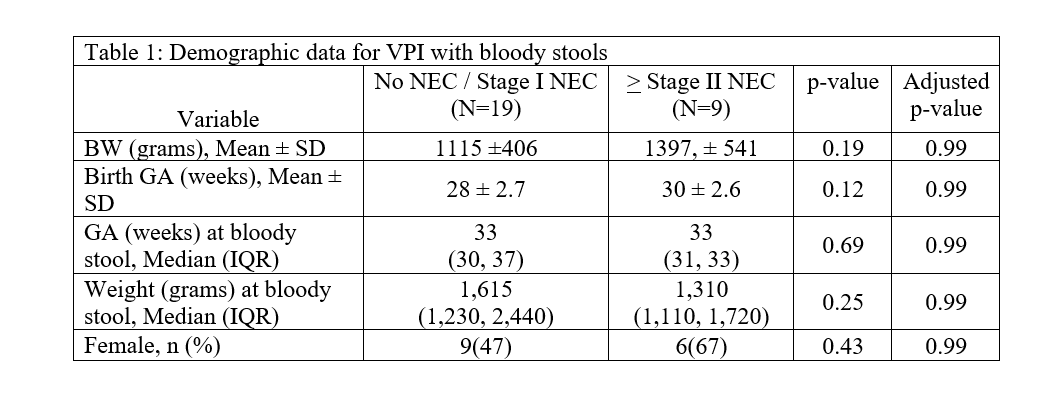
Background: Between 1 and 2% of NICU patients are reported to have blood in the stool during their hospitalization. Differentiating bloody stools due to NEC from other pathologies such as anal fissures, milk protein allergy, coagulopathy, and rare congenital GI anomalies can be challenging and contributes to antibiotic use in the NICU. Antibiotic stewardship data suggest increased antibiotic exposure for preterm infants increases the risk of NEC and bacteremia. Objective: To evaluate factors predictive of outcomes in newborns < 32 wks with bloody stools who underwent late onset sepsis (LOS) evaluation in the NICU. Design/Methods: This is a retrospective study at a regional referral level III NICU (ADC: 45, >700 annual admissions) of all very preterm infants (VPI) born ≤ 320/7 weeks GA who developed bloody stools and underwent a sepsis evaluation over a 10.5-year period (1/2013 - 6/2023). Patients were grouped and compared based on NEC stage (no NEC/stage I NEC vs Stage ≥ II NEC) Pearson chi-square/ Fisher's exact test was performed on all categorical variables; the Welch's two sample t-tests and Mann-Whitney-U tests were performed on continuous variables. The Benjamini-Yekutieli correction for multiple variables testing was performed and an adjusted p-value was calculated for each variable. Results: There were 7531 NICU admissions over 10.5 years, including 28 (0.4%) VPI who presented with a bloody stool: 19 (67.8%) without NEC or stage I NEC, and 9 (32.1%) with ≥ stage II NEC. Demographic data is presented in Table 1. Diagnoses for patients in the former group included stage I NEC (n=6, 31.6%), milk protein allergy (n= 2, 10.5%), anal fissure (n=1, 5.3%), rectal hematoma (n=1, 5.3%), and high phosphorous supplementation (n=1, 5.3%). No cause was identified for 7 (36.8%) of patients. Potential risk factors, physical exam findings, and laboratory data were similar between the two groups of infants with bloody stools (Table 2). None of the 28 VPI in either group had a positive blood culture.
Conclusion(s): No VPI with bloody stools were bacteremic over a 10.5-year period, and most of them (68%) did not have ≥ stage II NEC. These findings suggest antibiotic administration in this population is generally not warranted or beneficial.
Table 1: Demographic data for VPI with bloody stools
Table 2: Predictive factors for VPI with blood stools (no NEC/Stage 1 versus > Stage II NEC)

 photo")
.png)
