14 - Variation in NICU Practices for Parental Holding During Therapeutic Hypothermia
Friday, April 24, 2026
5:30pm - 8:00pm ET
Publication Number: 1012.14
Emma Elizabeth. Wiklund, Tufts University School of Medicine, Boston, MA, United States; Gloria D.. Sclar, The Barbara Bush Children's Hospital at Maine Medical Center, Portland, ME, United States; Elizabeth Scharnetzki, MaineHealth Institute for Research, Portland, ME, United States; Scott J. Evans, The Barbara Bush Children's Hospital at Maine Medical Center, Saco, ME, United States; Alexa Craig, Tufts University School of Medicine, Scarborough, ME, United States
Associate Professor of Pediatrics Tufts University School of Medicine Scarborough, Maine, United States
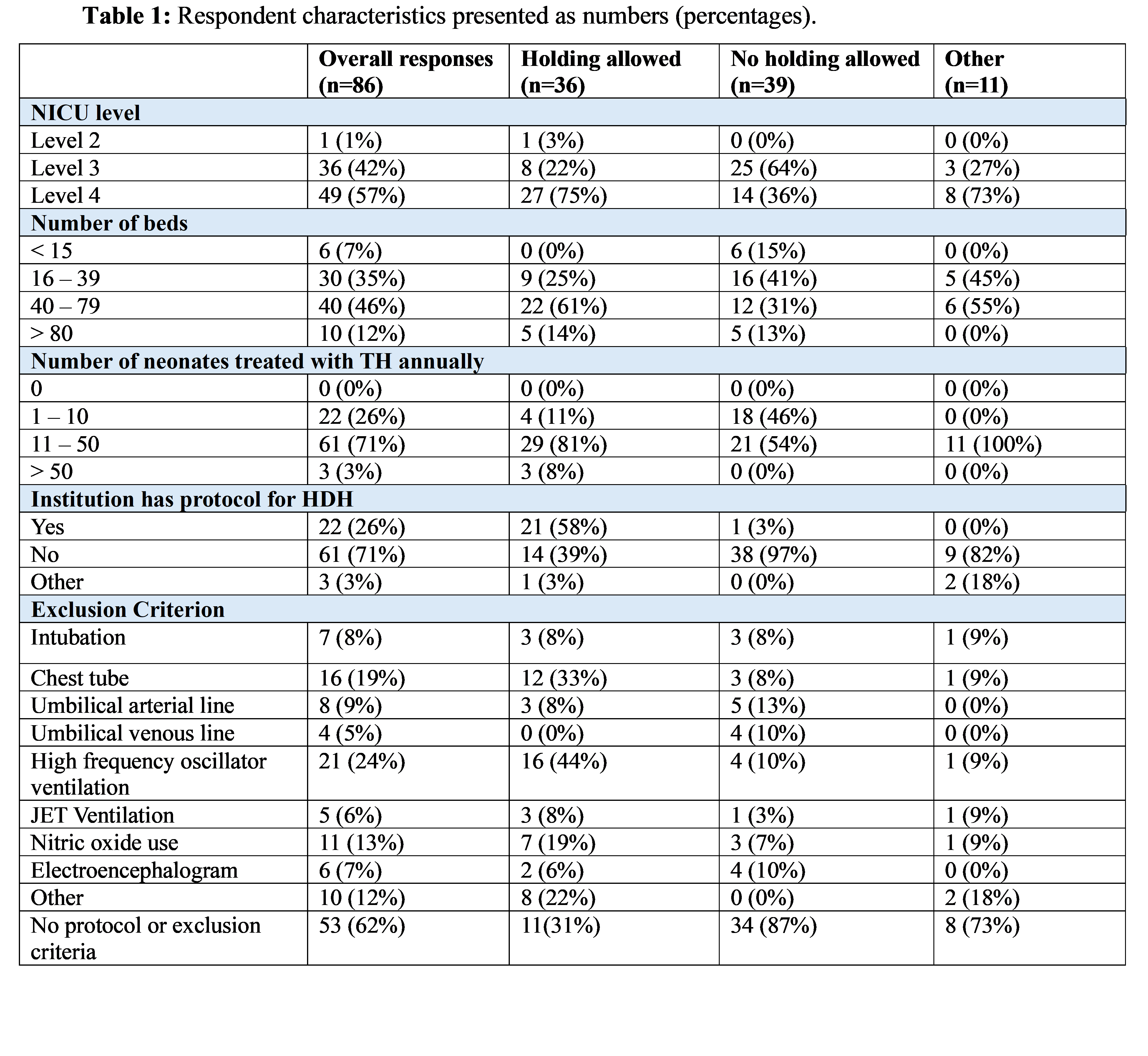
Background: Research has shown that it is feasible and safe for parents to hold their newborns during therapeutic hypothermia (TH), allowing for important early bonding. However, holding during TH has not been widely implemented across healthcare institutions. Objective: We surveyed clinicians to better understand the practice variation surrounding holding during TH. Design/Methods: A survey, designed by the research team, captured practices and requested protocols from those institutions that do practice holding. The survey was sent to all members of the Newborn Brain Society, the Child Neurology Society's Neonatal Special Interest Group, and additional clinicians that received the survey through chain-referral sampling. Summary statistics were calculated using descriptive statistics and protocols were analyzed using thematic analysis. Results: We received a total of 86 responses to the survey (Table 1). The majority of respondents represent level 4 NICUs with 40-79 beds who cool 11-50 babies annually. Of these respondents, 36 (42%) reported that the NICU they are employed at allows holding, 39 (45%) reported that their NICUs do not allow holding, and 11 (13%) answered "other" to indicate that their NICU had or were taking steps to implement holding. Of those who allow holding, 29/36 (81%) do not limit the duration of holding and 26/36 (72%) allow unlimited opportunities to hold. While the majority reported no formal exclusion criteria around holding, the most frequently cited exclusions were the presence of high frequency oscillator and chest tubes (Table 1). EEG leads, umbilical arterial lines, intubation, and JET ventilation were reported as exclusions by less than 10%.
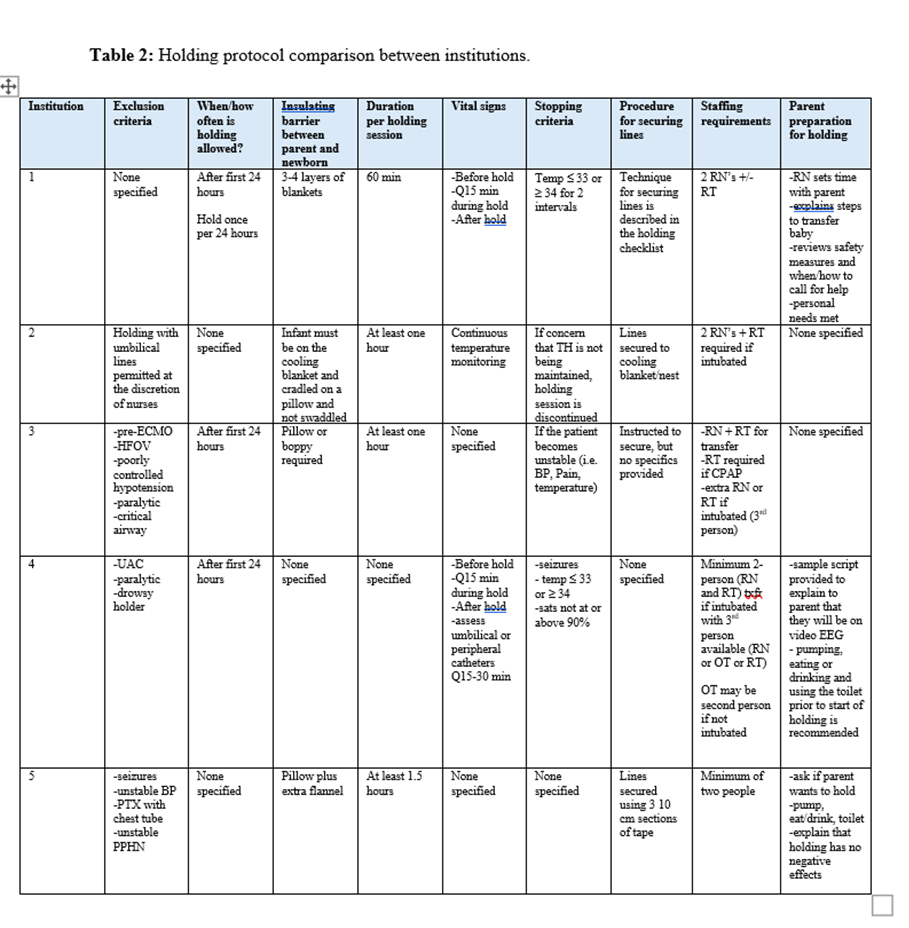
Of the respondents who work at a NICU that allows holding, 21/36 (58%) reported having a protocol to guide holding practices, but only 5 protocols were submitted by respondents. While there was significant variability between these 5 protocols, there was general agreement regarding allowing holding after 24-hours of life, a two-person minimum for transfer of newborn to parent, duration of one hour for holding, and clinical or temperature instability as a specified reason for stopping. Table 2 highlights the current variation of holding guidelines.
Conclusion(s): Our findings demonstrate limited implementation of parental holding during TH, as well as substantial variability among institutions that do practice holding. Therefore, future studies are warranted to define best practices for parental holding during TH to evaluate its impact on both clinical outcomes and the family experience.
Table 1: Respondent characteristics presented as numbers (percentages).
Table 2: Holding protocol comparison between institutions.

 photo")