645 - Immobilized Lipase Cartridge Improved Infant Growth with a Broad Range of Enteral Nutrition Practices
Friday, April 24, 2026
5:30pm - 8:00pm ET
Publication Number: 1622.645
Camilia R. Martin, Weill Cornell Medicine, New York, NY, United States; Lynn B. Wilson, Alcresta Therapeutics, Lakeville, MA, United States; Michael M.. Yeh, Alcresta Therapeutics, Waltham, MA, United States
Professor of Pediatrics Weill Cornell Medicine Chestnut Hill, Massachusetts, United States
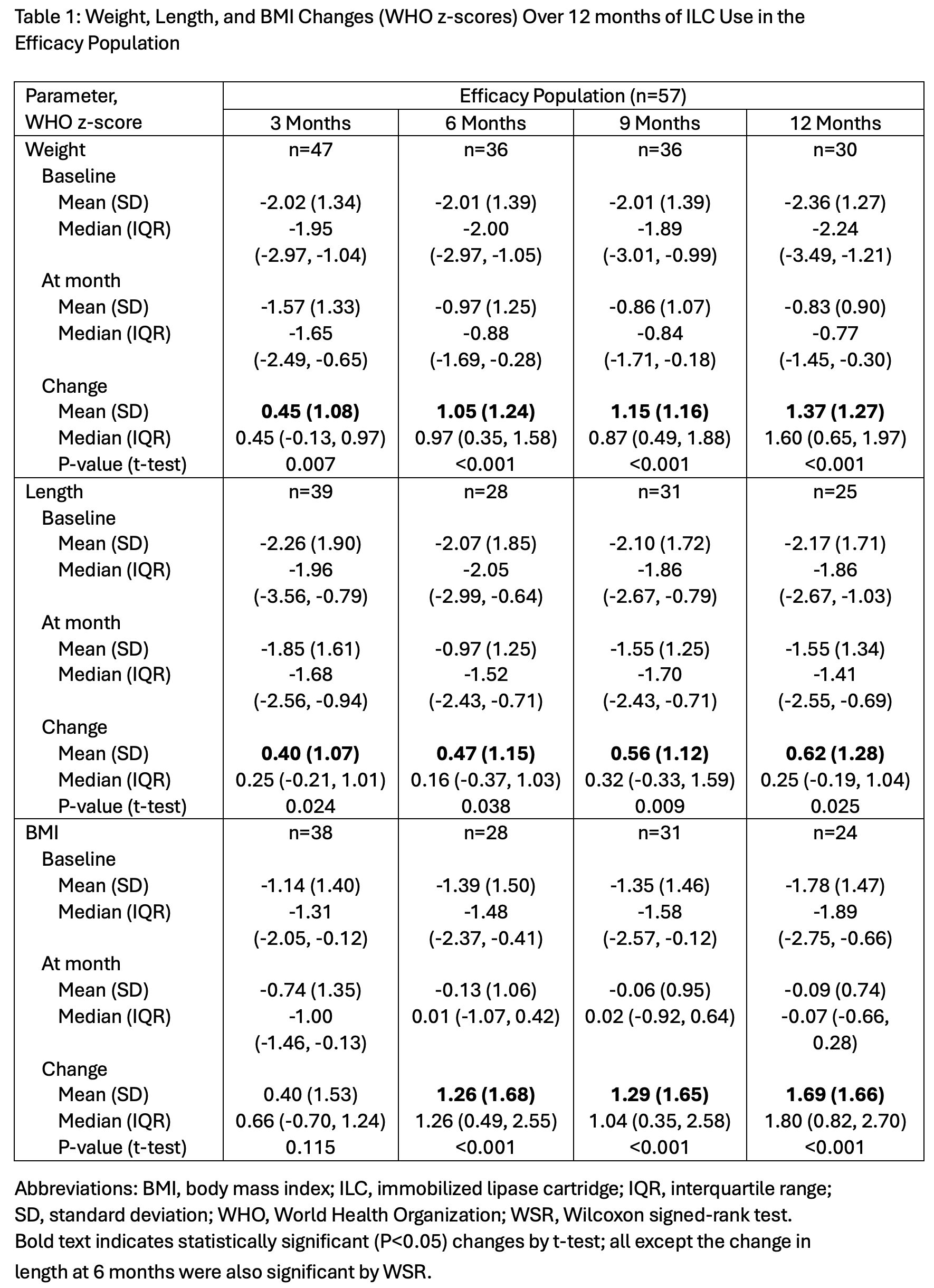
Background: Infants with medical conditions such as cystic fibrosis (CF), short bowel syndrome, and prematurity exhibit impaired fat digestion that contributes to suboptimal growth. A study in older subjects has shown that ex-vivo lipid hydrolysis of enteral formula or human milk using an immobilized lipase cartridge (ILC) can enhance fat absorption and thus may be an effective strategy to optimize growth in at-risk infants. Objective: To evaluate real-world growth outcomes, feeding practices, and safety among neonates and infants < 1 year initiating ILC with enteral nutrition (EN). Design/Methods: Retrospective analysis of de-identified data from a third-party reimbursement support database (Jan 2020-Oct 2024). Infants < 1 year initiating ILC with formula or human milk were included. Anthropometric measures were assessed using WHO growth standards. Safety was assessed by comparing complaint rates between infants and older ILC users. Results: Data from 96 infants across 60 U.S. centers were analyzed: mean age 5.64+3.57 months (age range -2.2 (adjusted age for prematurity) to 11.89 months). At initiation, 87% had CF, 40% were preterm, 47% had bowel resection, and 19% received parenteral nutrition. Feedings included formula only (87.5%) or human milk or fortified human milk (12.5%); 50% elemental, 33% polymeric, 17% semi-elemental. Caloric density ranged 20-30 kcal/oz; 70% had flow rates between 26-50 mL/hr; 25% continuous, 68% overnight feeds. Mean WHO z-scores for weight, length, and body mass index (BMI) improved significantly within 6 mo and continued to increase over 12 months (Table 1): weight -2.04 to -0.97 at 6 mo (p < 0.001) and -0.83 at 12 mo (p < 0.001); length -2.08 to -0.97 (p=0.038) at 6 mo and -1.55 (p=0.025) at 12 mo; BMI -1.30 to -0.13 (p < 0.001) at 6 mo. and -0.09 (p < 0.001) at 12 mo. Preterm and term infants achieved >1 WHO z-score gain by 6 mo. No device-related safety signals were identified.
Conclusion(s): ILC use in moderate preterm infants initiated after 2 months of age and in term infants with < 1 year of age was safe, well-tolerated, and associated with clinically meaningful improvements in growth parameters across a range of formulas, caloric densities, and delivery schedules. ILC provides a flexible and effective strategy to improve fat digestion and growth in infants with or at risk for fat malabsorption.
Table 1: Weight, Length, and BMI Changes (WHO z-scores) Over 12 months of ILC Use in the Efficacy Population

 photo")