567 - Airway anomalies in patients with 22q11.2 deletion admitted to the cardiac intensive care unit (CICU)
Friday, April 24, 2026
5:30pm - 8:00pm ET
Publication Number: 1544.567
Callie M. Cunningham, Cook Children's Medical Center, Dallas, TX, United States; Emily Lankford, Cook Children's Medical Center, Fort Worth, TX, United States; Lindsey Dodson, Cook Children's Medical Center, Fort Worth, TX, United States; Fadeke Ogunyankin, Cook Children's Health Care System, Fort Worth, TX, United States; Chris Tsao, Cook Children's Medical Center, Southlake, TX, United States; Lane T. Lanier, Cook Children's Medical Center, Fort Worth, TX, United States
Research Assistant/Medical Student Cook Children's Medical Center Dallas, Texas, United States
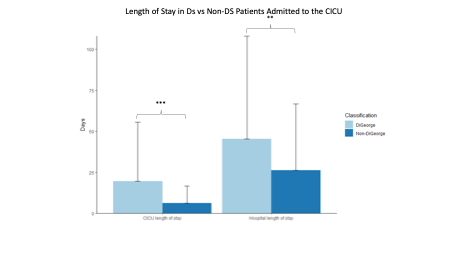
Background: While airway anomalies are not among the commonly emphasized features of DiGeorge Syndrome (DS) (22q11.2 deletion syndrome), structural abnormalities are reported to be frequent in patients undergoing otolaryngologic evaluation for aerodigestive symptoms. The overall prevalence of airway anomalies in patients with DS is not widely reported. We will describe the incidence of airway pathology in patients admitted to the CICU with DS. We hypothesize patients with DS require reintubation more frequently and have longer lengths of CICU and hospital stay than other children with the same cardiac diagnoses. Objective: To describe the incidence of airway evaluations and anomalies in the DS population in a single-center Cardiac Intensive Care Unit (CICU). Design/Methods: A retrospective review of 526 pediatric patients from 2018 to 2025 who underwent cardiac surgery and were admitted to the Cook Children's Cardiac Intensive Care Unit were analyzed. Genetic testing records confirmed diagnosis of 22q11.2 deletion. Demographic, surgical and outcomes data was used for comparative analysis. Results: Sixty-five patients with DS were included with 461 patients with congruent CHD without DS. Sixty-three patients underwent surgery. Due to electronic medical record transition, incomplete data points were omitted from data analysis. Twenty-nine DS patients (44%) had bronchoscopy with all having airway anomalies. Twelve patients with DS (18%) required airway surgery with 5 of those undergoing a second airway surgery during the CICU stay. Thirteen patients (21%) with DS required reintubation following surgery while 31 (6%) non-DS patients with the same CHD diagnosis required reintubation (p= < 0.05). Hours on mechanical ventilator support did not differ between the groups. CICU length of stay and hospital length of stay were significantly longer in the DS group than the non-DS group (p= < 0.05). There was no significant difference in mortality.
Conclusion(s): The incidence of airway anomalies in the DS population in the CICU is >40%. Patients with DS have a higher reintubation rate than their non-DS counterparts with the same cardiac diagnosis. CICU and hospital Length of stay in the DS population is longer than non-DS patients with the same cardiac diagnosis.
Figure 1: Cardiac ICU length of stay and total hospital length of stay for admission including CICU stay in patients with DS vs Non-DS
Airway Characteristics of DiGeorge Syndrome Patients (N=65) DS Table 2.pdf
Comparative data with Non-DiGeorge cardiac surgery patients (N=526) DS table 3.pdf