688 - Complicated Necrotizing Enterocolitis: Are the Outcomes Different from Preterm Infants with Perforated Necrotizing Enterocolitis - A Single Centre Retrospective Study
Friday, April 24, 2026
5:30pm - 8:00pm ET
Publication Number: 1665.688
Dwayne Mascarenhas, The Hospital for Sick Children, Toronto, ON, Canada; Ujjwala Mantha, University of Toronto Temerty Faculty of Medicine, Toronto, ON, Canada; Shravan Kanaparthi, The Hospital for Sick Children, Toronto, ON, Canada; Doaa Al-Dweik, The University of Western Ontario - Schulich School of Medicine & Dentistry, London, ON, Canada; Jordan Mann, The Hospital for Sick Children, Toronto, ON, Canada; Bonny Jasani, The Hospital for Sick Children, Toronto, ON, Canada
Staff Physician & Assistant Professor Mount Sinai Hospital, Toronto Toronto, Ontario, Canada
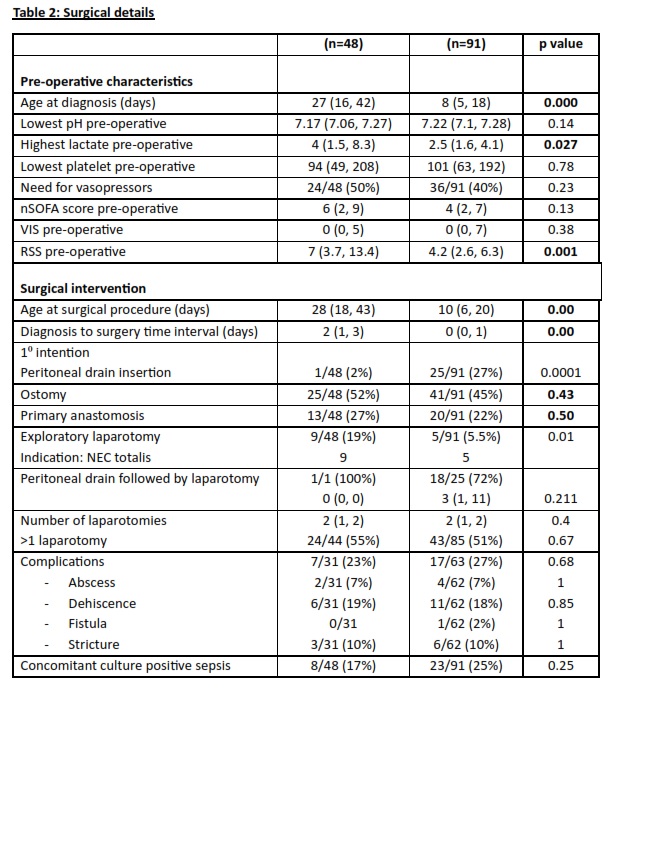
Background: Necrotizing enterocolitis (NEC) is a leading cause of morbidity and mortality in preterm infants. Distinguishing outcomes between complicated NEC (cNEC) and perforated NEC (pNEC) is essential to guide timely surgical decisions and improve prognosis. Objective: To compare the mortality, morbidities and short-term outcomes of cNEC versus pNEC in preterm infants undergoing surgical intervention. Design/Methods: We conducted a retrospective cohort study of preterm infants ≤30 weeks with Bell's stage 3A (cNEC) and 3B (pNEC) at a single quaternary neonatal intensive care unit between January 1, 2016 and June 30, 2024. The pre-specified outcomes included mortality, surgical interventions, nutritional outcomes, neonatal morbidities, anthropometric indices (weight, length, head circumference z-scores) at 36 weeks postmenstrual age. Mann-Whitney U test and Chi square test were used for comparing continuous and categorical data between the groups. Results: Of the 139 preterm infants with surgical NEC, 48 (35%) infants had cNEC and 91 (65%) infants had pNEC. The baseline characteristics, pre-operative characteristics, surgical intervention, neonatal morbidities, and nutritional and anthropometric outcomes are outlined in Tables 1-3. Compared to the pNEC group, the infants in the cNEC group were more likely to be female (58% vs 33%; p=0.004), older at diagnosis (27 vs 8 days; p=0.000), and had higher pre-operative lactate (4 vs 2.5; p=0.027) and pre-operative respiratory severity score (7 vs 4.2; p=0.001). Radiologically, the infants with cNEC were more likely to have bowel dilatation (87% vs 46%; p=0.000) and air-fluid levels (31% vs 8%; p=0.000) on abdomen xray, with no differences on abdomen ultrasound. Infants with cNEC were noted to have similar short-term clinical outcomes as pNEC (Table 3). Among the 63 infants who were initially diagnosed as cNEC, 15 (24%) infants developed a perforation. The other common indications for surgery included ischemic bowel loop [12 (%)] and worsening clinical status [11 (%)], with abdominal compartment syndrome having the highest mortality (Table 4).
Conclusion(s): Infants with cNEC present in majority of females, at a later post-natal age, have higher respiratory severity, unique radiologic characteristics, with time to surgery being 1-3 days. The progression of cNEC to surgical intervention underscores the need for vigilant monitoring of clinical indicators that predict deterioration and guide timely surgical decision-making.

 photo")
.jpg)
.jpg)
