Session: Neonatal Pulmonology - Clinical Science 2: Bronchopulmonary Dysplasia II
381 - Infants with Bronchopulmonary Dysplasia Discharged from the NICU with Chronic Non-Invasive Ventilation versus Ventilation via Tracheostomy
Friday, April 24, 2026
5:30pm - 8:00pm ET
Publication Number: 1365.381
Joseph D. Smits, University of Colorado School of Medicine, Denver, CO, United States; Kathleen E. Hannan, University of Colorado School of Medicine, Aurora, CO, United States; Emily Meneses, University of Colorado School of Medicine, Aurora, CO, United States; Christopher D. Baker, University of Colorado School of Medicine, AURORA, CO, United States; Satya Houin, University of Colorado School of Medicine, Aurora, CO, United States; Erica W. Mandell, University of Colorado School of Medicine, Aurora, CO, United States; Katelyn G. Enzer, University of Colorado School of Medicine, Aurora, CO, United States
Medical Student University of Colorado School of Medicine Denver, Colorado, United States
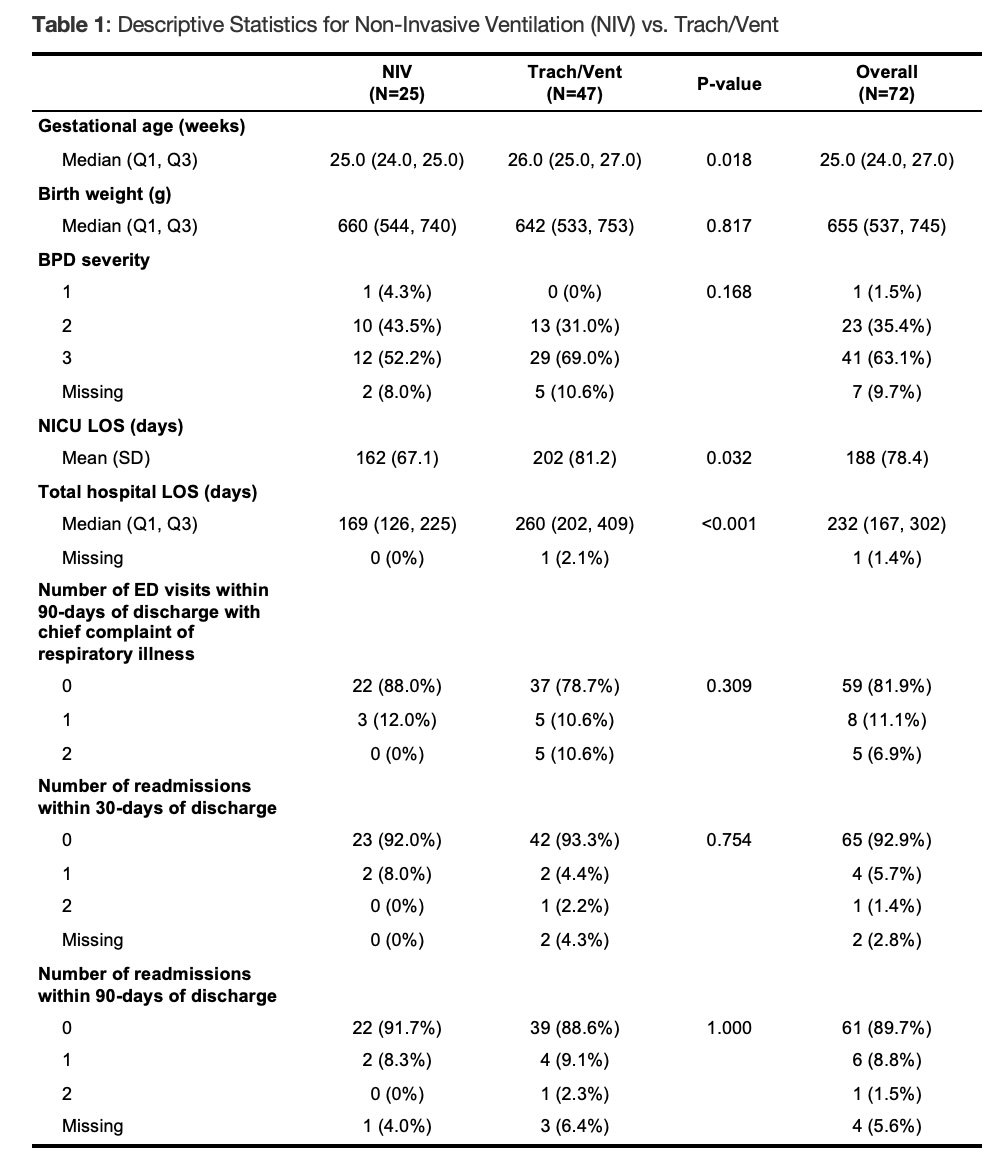
Background: With advances in neonatal care, the survival of extremely preterm infants has improved over the past several decades. Subsequently, the incidence of bronchopulmonary dysplasia (BPD), a form of chronic lung disease that is the most common sequelae of prematurity, has also increased. A select population of infants with BPD have severe lung disease that requires mechanical ventilation for many months or even years, posing a barrier to hospital discharge. Chronic ventilation can be provided via tracheostomy, which carries risk of complications and requires extensive education and monitoring by caregivers. Non-invasive ventilation (NIV) has also emerged as an option for long-term respiratory support, but there is limited data supporting home NIV for infants with BPD. Objective: Describe characteristics of infants with BPD discharged from the NICU with chronic ventilation via tracheostomies versus NIV. Outcomes analyzed included NICU and overall length of stay (LOS), 30- and 90-day readmissions, 90-day emergency room visits, and mortality. Design/Methods: This study was a single-center retrospective review comparing infants with BPD discharged with tracheostomy and mechanical ventilation versus NIV from 2020-2025 from a regional referral, Level IV NICU. Infants were eligible to discharge on NIV if they were on 2Lpm or less supplemental oxygen in the day and NIV at night. Infants were discharged home from the NICU or transferred to an inpatient floor for ongoing caregiver education. Data was collected by chart review. Comparisons were made using two-sample t-tests or Wilcoxon tests and chi-squared or Fisher's exact tests, as appropriate. Results: 72 infants were studied; 25 were discharged with NIV and 47 with tracheostomy. There was no significant difference in birth weight between the two groups, median gestational age was significantly lower for the NIV patients (p=0.02). Infants discharged on NIV had significantly shorter NICU LOS (162d vs 202d, p=0.03) and overall LOS (169d vs 260d, p< 0.001). Following discharge, there was no statistically significant difference in hospital readmissions at 30 or 90 days, emergency department visits at 90 days, or mortality (no mortality in either group).
Conclusion(s): When considering discharge for infants with BPD dependent on mechanical ventilation, NIV is a feasible and safe alternative for select infants. Further study is needed to explore optimal patient selection and outcomes.
Table 1: Descriptive Statistics for Non-Invasive Ventilation (NIV) vs. Tracheostomy Ventilation

 photo")