477 - It Takes Two: Getting to grips with two-handed neonatal mask ventilation in a simulation training programme
Friday, April 24, 2026
5:30pm - 8:00pm ET
Publication Number: 1457.477
Laura Ryan, National Maternity Hospital Dublin, Dublin 6W, Dublin, Ireland; Elizabeth H. Murphy, The National Maternity Hospital, Dublin, Dublin, Ireland; Carmel Maria. Moore, National Neonatal Tranport Team, Dublin, Dublin, Ireland; Linda Smiles, The National Maternity Hospital, Dublin, Dublin, Ireland; Anna Curley, NMH, dublin, Dublin, Ireland; Eoin O Currain, National Maternity Hospital, Dublin, Dublin, Ireland
Neonatal Research Fellow National Maternity Hospital Dublin Dublin 6W, Dublin, Ireland
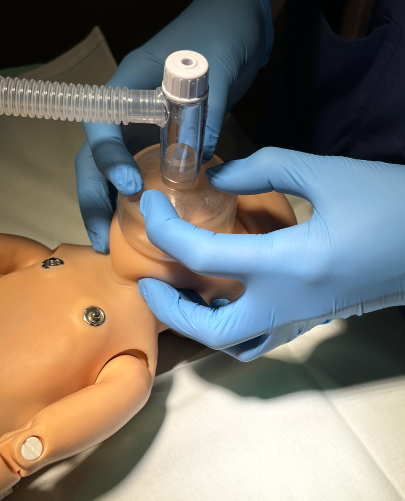
Background: Though effective facemask ventilation is essential in neonatal resuscitation, airway obstruction and mask leak are common. Evidence supports technique as the greatest factor controlling leak. Manikin-based studies and one pilot clinical study demonstrated reduced leak with two-handed hold, compared with one-handed. While mentioned by the Neonatal Resuscitation Programme (NRP), there is no requirement to receive instruction in or to demonstrate a two-handed mask hold, nor is it included in troubleshooting as part of MRSOPA. Prior to our randomised controlled trial, comparing mask leak in two versus one-handed hold in preterm and term neonates, we developed a training programme in mask ventilation with both handholds. Objective: To compare mask leak before and after training for two versus one-handed mask holds. Design/Methods: NICU clinicians were recruited and performed positive pressure ventilation (PPV) via a facemask on a term manikin attached to a respiratory function monitor. Initially, participants performed PPV for 30 seconds (blinded to the monitor) using one and two-handed mask holds. Following training they re-performed PPV using both mask holds. Mask leak, tidal volume, style of mask hold, hand preference, technique assessment and participant feedback were recorded. Results: 40 clinicians were enrolled (33% less than 1 year experience, 22% with 1-5 years, 45% with more than 5 years). Pre-training assessment demonstrated 82% of participants had minimal mask leak ( < 30%) with two-handed hold, compared to 47% with one-handed. Post-training, this increased to 93% vs 73% respectively (two vs one-handed mask hold). 65% preferred one-handed pre-training, which reduced to 37% post-training. Post-training, preference for two-handed increased to 50% and 13% had no preference. Participant feedback reported reduced cognitive load with a two-handed hold.
Conclusion(s): Mask leak remains a significant issue. This study highlights that, even without training, effective facemask ventilation in a manikin was more reliably achieved with a two-handed mask hold (82% prior to training, increasing to 93% after training). With a one-handed hold, less than half the participants (47%) demonstrated low leak prior to training, increasing to just 72% post-training. Feedback indicated increased participant preference for two-handed post-training, and reported an associated lower cognitive load. We await results of our RCT to inform how the holds compare in-vivo, and further simulation-based research to assess impact on cognitive load.

 photo")
.png)