507 - Time to Clinical Stability in Children with Medical Complexity Hospitalized with Pneumonia
Friday, April 24, 2026
5:30pm - 8:00pm ET
Publication Number: 1487.507
Francisco E. Herrera Carrillo, Boston Children's Hospital, Brookline, MA, United States; Jonathan Mansbach, Boston Children's Hospital, Boston, MA, United States; Kathleen D. Snow, Boston Children's Hospital, Boston, MA, United States
Research Boston Children's Hospital Brookline, Massachusetts, United States
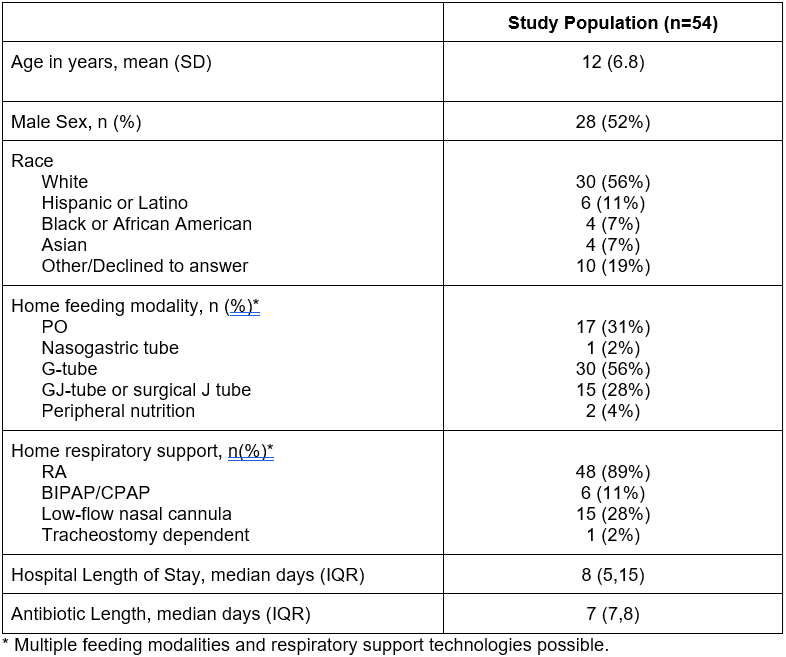
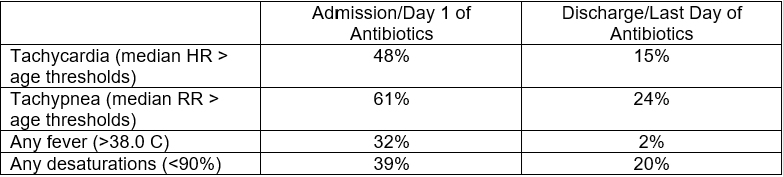
Background: Pneumonia is a common reason for hospitalization among children with medical complexity (CMC). However, limited studies have characterized physiologic recovery patterns in CMC with pneumonia. Objective: Our objective was to use vital signs over the course of the hospitalization to define time to clinical stability and discharge readiness among CMC hospitalized with pneumonia. Design/Methods: We conducted a retrospective cross-sectional study of children age 2-25 years with ≥ 3 underlying chronic medical conditions and a diagnosis of pneumonia (presumed bacterial) hospitalized on an inpatient medical floor between January 2022 to December 2023. We extracted heart rate [HR], respiratory rate [RR], temperature [T] and oxygen saturation [SpO2] from the electronic medical record. Median HR, RR, T, and SpO2 were computed for each 24-hour calendar day from the start of antibiotics through antibiotic completion or hospital discharge. We defined clinical stability as the first hospital day all the following criteria were met: median HR and RR < 99th percentile for age, T < 38.0ºC, and SpO2 ≥ 90%. We then calculated the difference between time to clinical stability [TCS] and length-of-stay [LOS] for each patient. Kaplan-Meier curves for TCS and LOS were compared using the log-rank test. Results: We included 54 CMC hospitalized for pneumonia (Table 1). Tachypnea (61%) and tachycardia (48%) were the most frequent abnormalities on admission (Table 2). Vital signs improved from admission to discharge with median decreases in HR (-20 bpm), RR (-4 breaths/min), and temperature (−0.2 °C), and median SpO2 increase (+.75 %). However, 46% had at least one unstable vital sign at discharge. Median TCS was 3 days (IQR 2-4), median antibiotic duration was 7 days (IQR 7-8), and median LOS was 8 days (IQR 5-15). Kaplan-Meier curve (Figure 1) demonstrated that physiologic stability was reached significantly earlier than discharge (P=0.034). Overall, 78% of our cohort remained hospitalized ≥ 1 day after achieving clinical stability (median LOS-TCS difference = 5 days [IQR 2-12]).
Conclusion(s): Although most CMC hospitalized for presumed bacterial pneumonia achieved physiologic stability within 4 days, 50% had a LOS that was twice as long. While non-pneumonia factors (e.g., underlying comorbidity, social determinants of health) may be related to LOS, this pattern supports trialing shorter antibiotic durations in select CMC. In a population that has frequent antibiotic courses, using vital-sign-based stability criteria to guide and personalize length of antibiotic therapy may be beneficial.
Table 1. Patient Demographics and Hospitalization Characteristics of Study Population
Table 2. Proportion of patients with unstable vital signs at antibiotic initiation and completion
Figure 1. Kaplan-Meier analysis comparing time to clinical stability (TCS) and length of stay (LOS) among children with complex medical conditions hospitalized for pneumonia

 photo")
.png)
