306 - Ear-resistable: Family Engagement with an AI-Enabled Otoscope Study
Friday, April 24, 2026
5:30pm - 8:00pm ET
Publication Number: 1292.306
Grzegorz Zapotoczny, Ann & Robert H. Lurie Children's Hospital of Chicago, Chicago, IL, United States; Oluwadamilola Ibrahim, Ann & Robert H. Lurie Children's Hospital of Chicago, Chicago, IL, United States; Juan C. Espinoza, Ann & Robert H. Lurie Children's Hospital of Chicago, Chicago, IL, United States
Assistant Professor of Pediatrics Ann & Robert H. Lurie Children's Hospital of Chicago Chicago, Illinois, United States
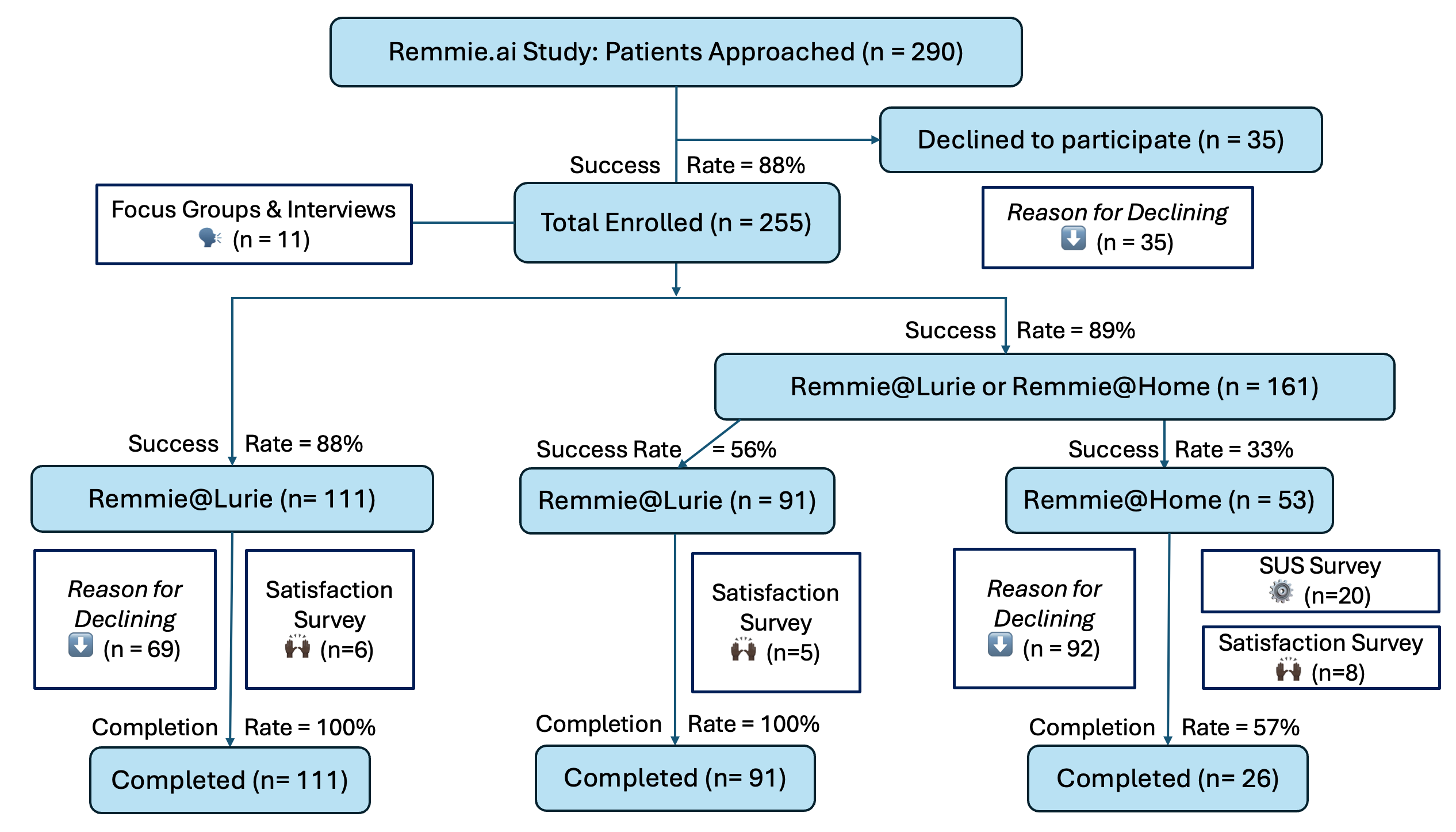
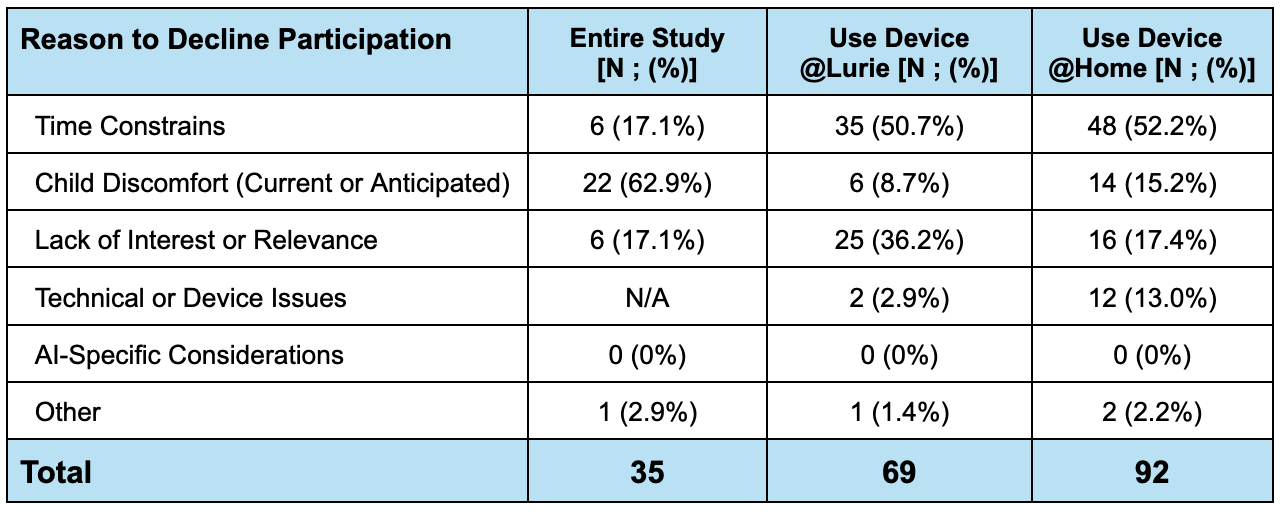
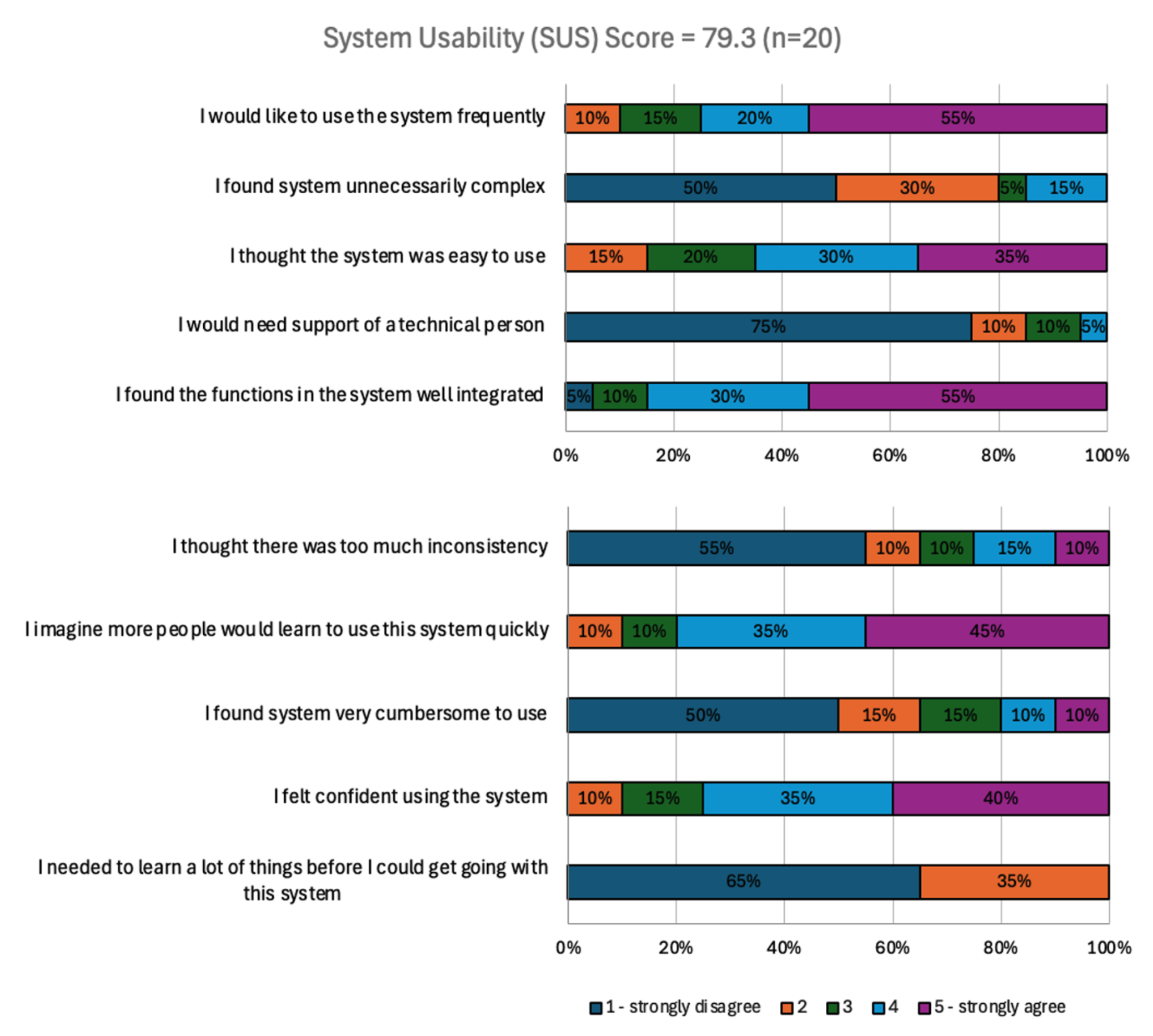
Background: Artificial Intelligence (AI) in healthcare is promising, but parents often raise valid concerns about privacy, safety, bias, and how AI will be used in decisions about their children. These concerns, along with technical hurdles and the high data demands of AI, can hinder adoption. Researchers face similar concerns when enrolling patients in studies about or with AI technologies. We examined family engagement and attitudes towards participating in a federally-funded study of an AI-enabled medical device. Objective: To evaluate patient family engagement and attitudes towards AI research as a part of the NIH SBIR-funded study for the development of an AI-enabled otoscope intended for clinical decision support. Design/Methods: Between Dec 2024 and Nov 2025 we recruited 290 participants for the prospective Remmie.ai image collection study (IRB # 2024-6966). We offered to collect feedback from patients who declined to participate (brief interviews), enrolled in the study (focus groups; satisfaction surveys), and who took the device home (system usability surveys). Quantitative and qualitative data elements were summarized using descriptive statistics. Results: Of the 290 patients approached, we enrolled 255 (88%; Figure 1). The most cited reasons to decline study participation were child discomfort (62.9%), time constraints (17.1%) and lack of interest (17.1%). Participants who enrolled but did not wish to test Remmie.ai also indicated time constraints and lack of interest, but only 20/161 (12.4%) expressed child discomfort concerns (Table 1). Of the 20 participants who took the device home, 5% expressed a strong preference for the immediate AI feedback, while 65% preferred to wait up to 24h clinician feedback; 30% had no preference. Of the 19 participants who filled out a 10-question satisfaction survey, Remie@Lurie and Remmie@Home respondents scored respectively 97.2% and 77.5% questions (n=190) favorably (Likert scale 4 or 5). The @Home participants scored Remmie.ai usability at 79.3 (Figure 2; Grade A- ; Excellent). None of the participants expressed strong concerns regarding the AI component.
Conclusion(s): High enrollment indicates that families are willing to engage in AI research when safeguards are clear and children's wellbeing is protected. While participants reported few AI-specific concerns, they consistently preferred clinician-mediated feedback over immediate AI output. Together, these findings suggest that clinician-in-the-loop designs and transparent communication can convert general AI wariness into research participation.
Figure 1. Consort diagram illustrating Remmie.ai study enrollment at Lurie Children's Hospital of Chicago.
Table 1. Patterns of AI Research Participation Hesitancy.
Figure 2. Remmie.ai System Usability Survey Results. Legend: System Usability Score (SUS) Scale: 84.1 to 100 (Grade A+ ; Best Imaginable) ; 80.8 to 84.0 (Grade A ; Excellent) ; 78.9 to 80.7 (Grade A- ; Excellent) ; 77.2 to 78.8 (Grade B+ ; Excellent) ; 74.1 to 77.1 (Grade B ; Good) ; 72.6 to 74.0 (Grade B- ; Good) ; 71.1 to 72.5 (Grade C+ ; Good) ; 65.0 to 71.0 (Grade C ; Okay) ; 62.7 to 64.9 (Grade C- ; Okay) ; 51.7 to 62.6 (Grade D ; Okay) ; 0 to 51.6 (Grade F; Poor)

 photo")
 Legend:
Legend: