397 - Relative Effectiveness and Public Health Impact of Cell-Based Versus Egg-Based Quadrivalent Influenza Vaccines Across Paediatric Populations During the 2023–24 Influenza Season in the United States
Saturday, April 25, 2026
3:30pm - 5:45pm ET
Publication Number: 2386.397
Alicia N. Stein, CSL Seqirus, Melbourne, Victoria, Australia; Anusorn Thanataveerat, Veradigm, Elmhurst, NY, United States; Kimberly McDermott, Veradigm, Hingham, MA, United States; Alex Dean, Veradigm, San Francisco, CA, United States; Stephanie Wall, Veradigm, Chicago, IL, United States; Cory Pack, Veradigm, Santa Barbara, CA, United States; Ian McGovern, CSL Seqirus, Quincy, MA, United States; Sheena Sullivan, Monash University, Melbourne, Victoria, Australia; Mendel Haag, CSL Seqirus, Amsterdam, Noord-Holland, Netherlands
Associate Director, RWE CSL Seqirus Quincy, Massachusetts, United States
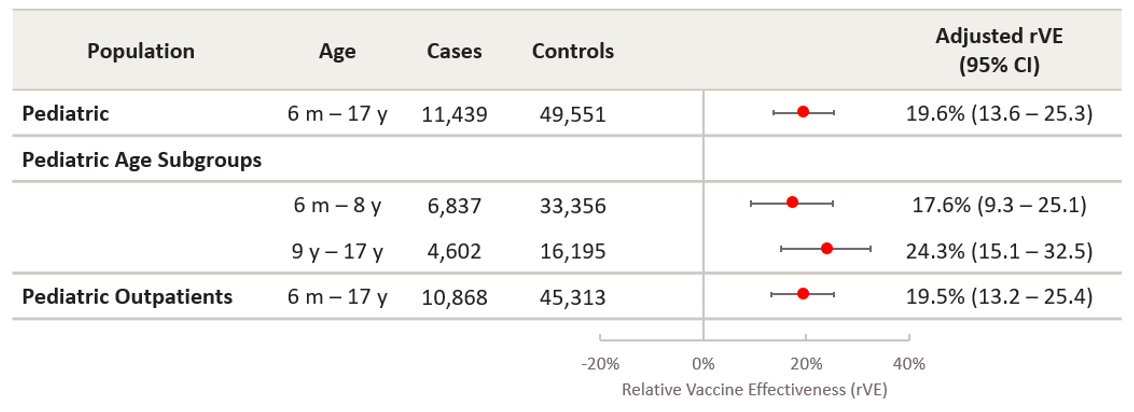
Background: Egg-adaptive mutations occurring during egg-based influenza vaccine manufacturing can alter the antigenicity of the vaccine virus, contributing to reduced effectiveness. Previous studies demonstrated improved effectiveness of cell-based (QIVc) versus egg-based (QIVe) quadrivalent influenza vaccines against test-confirmed influenza in populations aged 4 to 64 years during the 2017-18 to 2019-20 influenza seasons and aged 6 months to 64 years during the 2022-23 season in the United States. Objective: With increasing uptake of QIVc in the pediatric population, we aimed to estimate the relative vaccine effectiveness (rVE) of QIVc versus QIVe against test-confirmed influenza during the 2023-24 season in the US, including analysis in subpopulations defined by age. Design/Methods: We used linked data combining electronic health records, medical and pharmacy claims, and laboratory tests from multiple sources in the United States. A retrospective test-negative design was applied among individuals aged 6 months to 64 years vaccinated with either QIVc or QIVe in 2023-24, who had an influenza test obtained within 7 days of an acute respiratory or febrile illness. rVE was estimated using a doubly robust logistic regression analysis. Here we present results obtained in the full pediatric population aged 6 months to 17 years and subpopulations from age 6 months to 8 years, 9 to 17 years and in outpatient setting only. The public health impact in the full pediatric population was estimated using a compartmental influenza burden-averted model. Results: The dataset included 60,990 vaccinated and influenza-tested pediatric patients, of whom 7,194 (11.8%) received QIVc and 53,796 (88.2%) received QIVe. QIVc was significantly more effective than QIVe in preventing test-confirmed influenza in the full pediatric population, with an estimated rVE of 19.6% (95% CI: 13.6-25.3%). Consistent rVE results were observed across both pediatric age subgroups and in the outpatient setting (Figure 1). If all vaccinated individuals aged 6 months-17 years in the US received QIVc over QIVe, an additional estimated 1,072,376 symptomatic illnesses would have been prevented, with proportionate reductions in related complications (Table 1).
Conclusion(s): This study demonstrates superior effectiveness of QIVc compared to QIVe in preventing test-confirmed influenza in pediatric populations during the 2023-24 season in the United States. Substantial influenza burden could be prevented by use of cell-based instead of egg-based influenza vaccines in the pediatric population.
Figure 1: Adjusted relative vaccine effectiveness of cell-based (QIVc) versus egg-based (QIVe) quadrivalent influenza vaccines against test-confirmed influenza
Table 1: Estimated influenza burden averted by use of QIVc vs QIVe in subjects 0-17 years in the United States 2023-24 influenza season


.png)
