540 - Neighborhood Social Vulnerability and Pediatric Asthma Utilization: A Retrospective Cohort Study in Hamilton County, Ohio
Saturday, April 25, 2026
3:30pm - 5:45pm ET
Publication Number: 2525.540
Reshma Sabnani, Cincinnati Children's Hospital Medical Center, Cincinnati, OH, United States; Ryan Murphy, Cincinnati Children's Hospital Medical Center, Cincinnati, OH, United States; Yin zhang, Cincinnati Children's Hospital Medical Center, West Chester, OH, United States; Cole Brokamp, University of Cincinnati College of Medicine, Cincinnati, OH, United States; Andrew F. Beck, Cincinnati Children's Hospital Medical Center, Cincinnati, OH, United States; E. Melinda Mahabee-Gittens, Cincinnati Children's Hospital Medical Center, Cincinnati, OH, United States
Clinical Pediatric Emergency Medicine Fellow Cincinnati Children's Hospital Medical Center Cincinnati, Ohio, United States
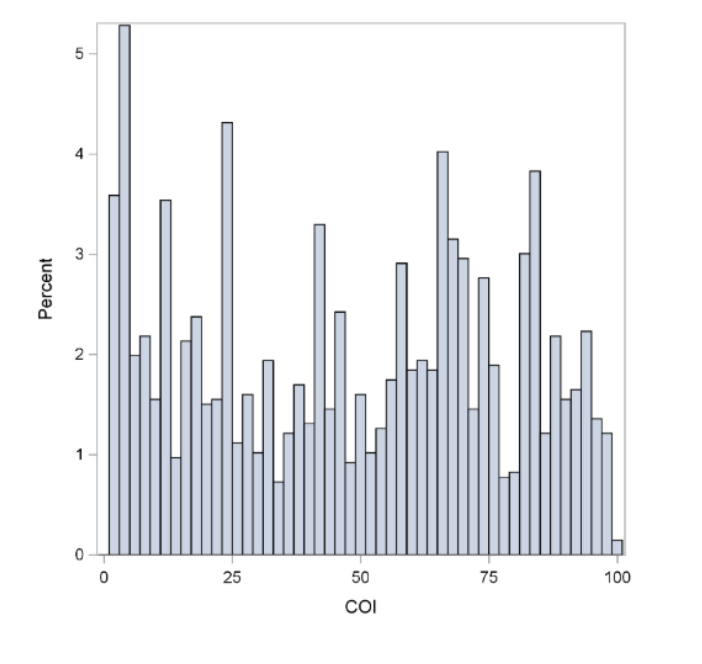
Background: Asthma is a leading cause of pediatric emergency department (ED) and urgent care (UC) acute visits nationwide and contributes substantially to morbidity, school absenteeism, caregiver work loss, and healthcare costs. In Greater Cincinnati, pediatric asthma hospitalizations occur at rates nearly three times the national average. Objective: To examine the association between census tract-level social vulnerability indices-including the Child Opportunity Index (COI), Community Material Deprivation Index (DI), and Social Vulnerability Index (SVI)-and the frequency of pediatric asthma-related ED and UC visits and revisits. Design/Methods: We conducted a retrospective observational study using electronic health record data from children aged 2-18 years residing in Hamilton County, Ohio. Eligible patients had an ED or UC index visit for asthma between December 2023 and December 2024. Residential addresses were geocoded to census tracts and linked with tract-level COI, DI, and SVI scores. Patients were followed for nine months after the index visit to assess revisit rates. Results: Among 2,230 patients that visited the ED/UC for acute asthma exacerbations, 473 (21%) revisited within 9 months 1,360 (61%) were male and 870 (39%) were female; 45% were White, 41% Black, and 14% Other. Most had public insurance (59%), followed by private insurance (37%), and no insurance (4%). Patients were divided into quartiles based on neighborhood indices. For ED/UC initial visits for asthma, COI and SVI were fairly evenly distributed, as per Figure 1 and Figure 2. In contrast, DI was skewed suggesting fewer initial visits from higher deprivation areas as per Figure 3. Patients in high-vulnerability areas (low COI, high DI/SVI) had more ED/UC revisits. Every 10% increase in COI was associated with a 3.5% decrease in revisits. Every 10% increase in SVI was associated with a 4.1% increase in revisits, and every 10% increase in DI was associated with a 0.67% increase in revisits.
Conclusion(s): Although children's initial visits to the ER/UC for acute asthma are typically independent of COI and SVI, the rate at which they revisit is significantly influenced by these indices suggesting that acute pediatric asthma reutilization is significantly associated with neighborhood-level social vulnerability. These findings underscore the importance of geographically targeted, equity-focused interventions to reduce asthma burden in high-risk communities.

.png)
.png)
