344 - Neurodevelopmental Outcomes in Patients with Severe Bronchopulmonary Dysplasia with and without a Tracheostomy
Saturday, April 25, 2026
3:30pm - 5:45pm ET
Publication Number: 2333.344
Lakeya O'Neal, University of Tennessee Health Science Center College of Medicine, Memphis, TN, United States; Mark F. Weems, University of Tennessee Health Science Center, Memphis, TN, United States; Megan Derrer, University of Tennessee Health Science Center, Memphis, TN, United States; Toni M. Whitaker, University of TN Health Science Center, Le Bonheur Children's Hospital, Memphis, TN, United States; Mohamad Elabiad, University of Tennessee Health Science Center, Memphis, TN, United States; Divya Rana, University of Tennessee Health Science Center College of Medicine, Memphis, TN, United States
Fellow University of Tennessee Health Science Center College of Medicine Memphis, Tennessee, United States
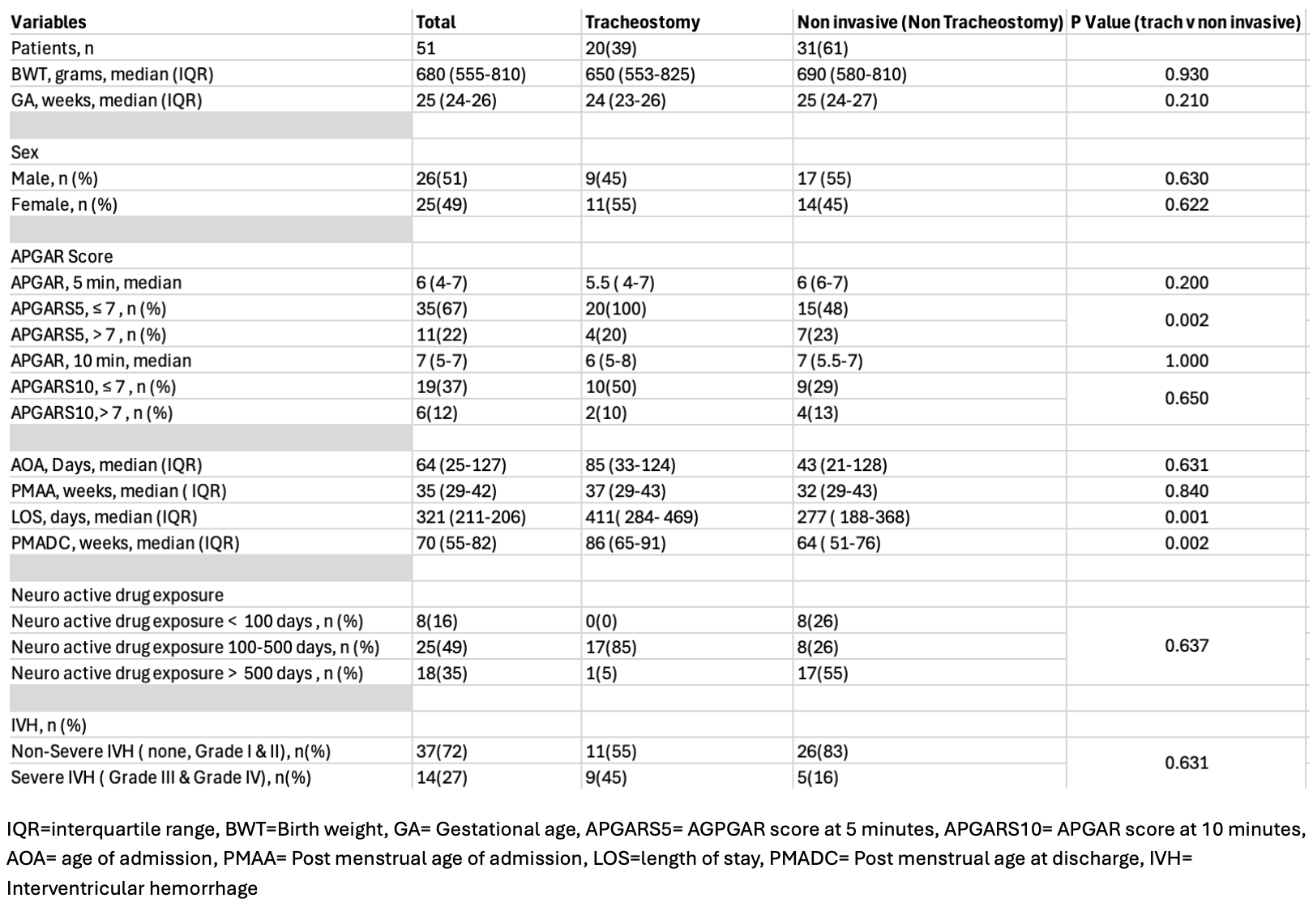
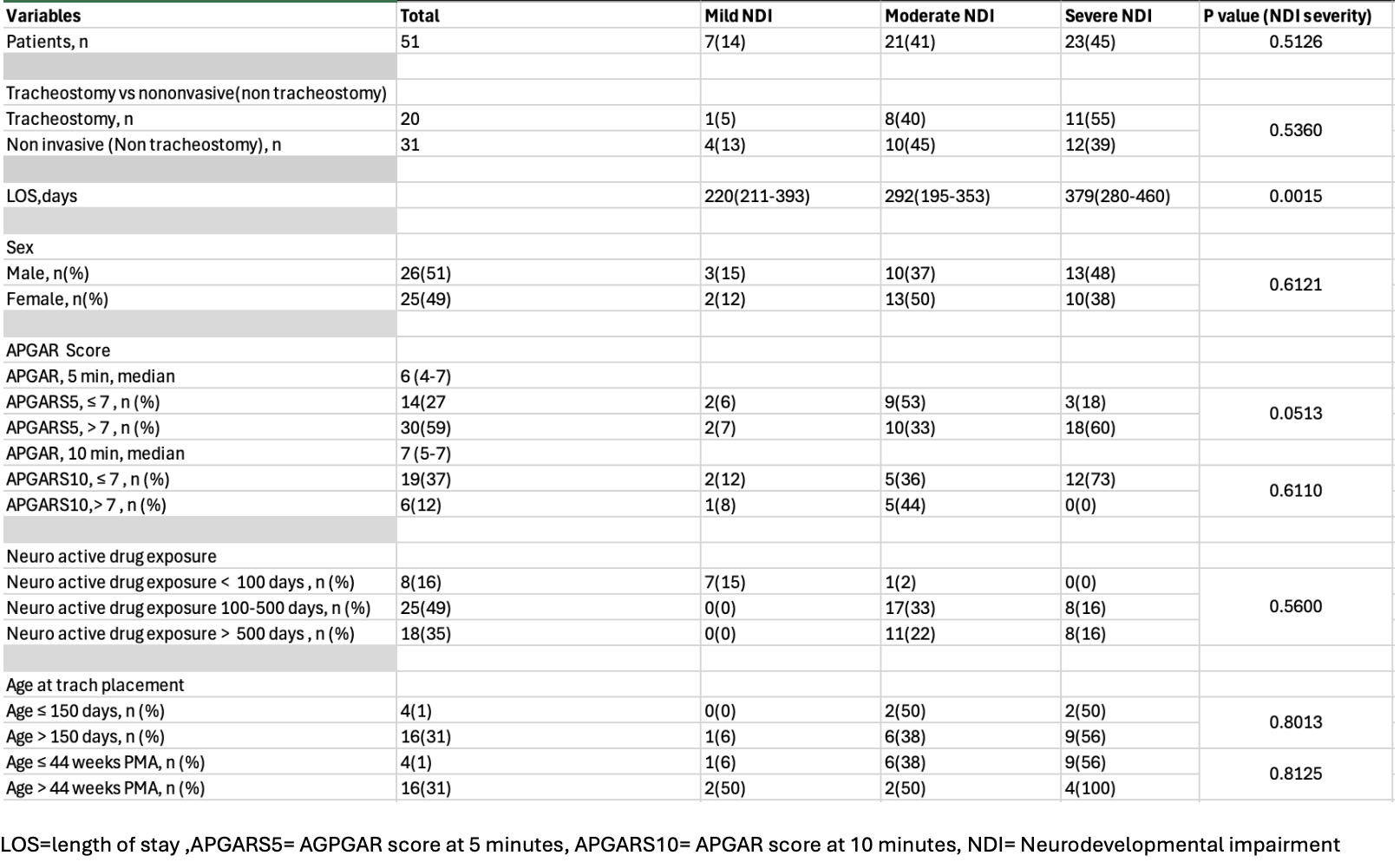
Background: Bronchopulmonary dysplasia and neurodevelopment outcomes have been a challenge for many years in the neonatal intensive care unit.Often times, these patients have prolonged stays which limit their ability to be in natural surroundings to promote typical development.Research has continued to show that patients have developmental delays upon discharge, and it has been shown that severe BPD and prolonged ventilation are associated with poor neurodevelopmental outcomes.Moreover, patients are on different respiratory support modes during their hospital stay and that can create different challenges developmentally. Objective: Assess the association between neurodevelopmental outcomes in tracheostomy and non-invasive respiratory support to determine if there is a difference in developmental outcomes between the two groups. Design/Methods: This retrospective study includes all neonates with grade III BPD (Jensen et al. Am J Respir Crit Care Med, 2019) managed in our NICU from January 1,2020, to December 31, 2024.Patients were excluded if they died before NICU discharge, if they were still in-patient at study end date, if they had genetic disorders, no outpatient follow up visit, or an abnormal head ultrasound associated with developmental impairment.The inclusion criteria was patients with Grade III BPD (definition still intubated at 36 w/Ginseng criteria), < 32 weeks birth GA ,> 36 weeks requiring respiratory support, any clinic visit neurodevelopmental assessments up to 1 year. The chi squared test using STATA was used to analyze the categorical data and if a p value was < 0.05 that expressed that there was a statistical significance. Results: During this study period, 51 patients were included.Table 1 shows data grouped by placement of tracheostomy vs non-tracheostomy.Tracheostomy placement was associated with a longer length of stay[411 (IQR 284-469) vs 277 (188-268) days, p=0.001].Table 2 reports data grouped by mild, moderate, and severe neurodevelopmental impairment (NDI). Severe NDI was also associated with a longer length of stay [379 (280-460) days, compared with moderate NDI 292 (195-353) and mild NDI 220 (211-393),p=0.0015].However, tracheotomy placement was not associated with differences in NDI (p=0.53).
Conclusion(s): Patients with a tracheostomy that required long term ventilation to discharge home did not show improved neurodevelopmental outcomes compared to the non tracheostomy group.Overall, this study showed that the tracheostomy group was associated with older age at discharge and longer length of stay, which could correlate with poor neurodevelopmental outcomes.